Vous aimerez peut-être aussi
- Malabsorption SyndromeDocument24 pagesMalabsorption SyndromeanojanPas encore d'évaluation
- Approach To Malabsorption (SANJAY)Document58 pagesApproach To Malabsorption (SANJAY)Sanjay KumarPas encore d'évaluation
- Chronic Diarrhea and Malabsorption: Causes and TreatmentDocument25 pagesChronic Diarrhea and Malabsorption: Causes and TreatmentadelekeyusufPas encore d'évaluation
- Malabsorption Syndromes in Children PDFDocument6 pagesMalabsorption Syndromes in Children PDFkoreswilsonPas encore d'évaluation
- Disorders of Intestinal AbsorptionDocument83 pagesDisorders of Intestinal AbsorptionMalika SadridinovaPas encore d'évaluation
- Malabsorption Syndrome: Causes, Symptoms and TreatmentDocument5 pagesMalabsorption Syndrome: Causes, Symptoms and TreatmentPriyaPas encore d'évaluation
- Malabsorption SyndromeDocument12 pagesMalabsorption Syndromekint manlangitPas encore d'évaluation
- Malabsorption SyndromesDocument29 pagesMalabsorption SyndromesuouoPas encore d'évaluation
- Steatorrhea: Section A2/ Group IvDocument43 pagesSteatorrhea: Section A2/ Group IvKristian Cada100% (4)
- Digestive System Disorder AssessmentDocument50 pagesDigestive System Disorder AssessmentTaate MohammedPas encore d'évaluation
- نسخة Malabsorption 10Document41 pagesنسخة Malabsorption 10نوف الحربي.Pas encore d'évaluation
- Irritable Bowel Syndrome Malabsorption SyndromeDocument29 pagesIrritable Bowel Syndrome Malabsorption SyndromeLiza Marie IgnacioPas encore d'évaluation
- PancreasDocument20 pagesPancreasnarendramedaPas encore d'évaluation
- Aminacid MetabolismDocument84 pagesAminacid MetabolismAaronJose100% (1)
- Diseases of Small Intestine MHMDocument15 pagesDiseases of Small Intestine MHMNa DaPas encore d'évaluation
- Malabsorption SyndromeDocument3 pagesMalabsorption SyndromeAna Irda100% (1)
- 31.chronic Diarrhea and MalabsorbtionDocument14 pages31.chronic Diarrhea and MalabsorbtionSajjal AliPas encore d'évaluation
- Fecal AnalysisDocument23 pagesFecal AnalysisBabylene MamauagPas encore d'évaluation
- Exmd 509 Mcgill ClassDocument47 pagesExmd 509 Mcgill ClassSora OhPas encore d'évaluation
- Parenteral Nutrition-Associated Liver Disease: ReviewDocument4 pagesParenteral Nutrition-Associated Liver Disease: ReviewdhirazhrPas encore d'évaluation
- Malabsorption SyndromeDocument31 pagesMalabsorption SyndromeSahilSharma100% (1)
- Fat MalabsorbtionDocument18 pagesFat MalabsorbtionDragosAurPas encore d'évaluation
- Disorders of Small IntestineDocument41 pagesDisorders of Small IntestineSamuel kuriaPas encore d'évaluation
- GI Disorders Note - 221206 - 074045Document48 pagesGI Disorders Note - 221206 - 074045Shabnam SajidaPas encore d'évaluation
- Steatorrhea Medical Biochemistry ReportDocument72 pagesSteatorrhea Medical Biochemistry ReportDey Sibal80% (5)
- 1.CBE CME Obstructive JaundiceDocument39 pages1.CBE CME Obstructive JaundicedeepikaPas encore d'évaluation
- Malabsorption syndrome nursing careDocument27 pagesMalabsorption syndrome nursing careShitaljit IromPas encore d'évaluation
- Persistent Diarrhoea & Chronic DiarrhoeaDocument34 pagesPersistent Diarrhoea & Chronic DiarrhoeanilmbbsPas encore d'évaluation
- Extrahepatic Biliary Tract Pathology - Cholidolithiasis, Cholidocholithiasis, Cholecystitis and CholangitisDocument60 pagesExtrahepatic Biliary Tract Pathology - Cholidolithiasis, Cholidocholithiasis, Cholecystitis and CholangitisDarien LiewPas encore d'évaluation
- Approach To GI DisordersDocument28 pagesApproach To GI DisordersdrvivekshimlaPas encore d'évaluation
- CHOLELITHIASISDocument13 pagesCHOLELITHIASISMaria Nadeem, BS Home Economics Student, UoPPas encore d'évaluation
- Git Lecture 4Document8 pagesGit Lecture 4Heersh raofPas encore d'évaluation
- Disorders of digestion and absorption of carbohydratesDocument34 pagesDisorders of digestion and absorption of carbohydratesSanjeev WalvekarPas encore d'évaluation
- Management of Renale Disease-1Document20 pagesManagement of Renale Disease-1Abdur RehmanPas encore d'évaluation
- IBS: A Guide to Irritable Bowel SyndromeDocument38 pagesIBS: A Guide to Irritable Bowel SyndromeMuhammed sherbinPas encore d'évaluation
- Report DISORDERS OF MALABSORPTIONDocument8 pagesReport DISORDERS OF MALABSORPTIONKathleen Anzhelika B. NemenzoPas encore d'évaluation
- CHOLELITHIASISSDocument29 pagesCHOLELITHIASISSAngelica Mercado SirotPas encore d'évaluation
- Malabsorption SyndromeDocument1 pageMalabsorption SyndromesamanthaPas encore d'évaluation
- Malabsorption SyndromeDocument15 pagesMalabsorption SyndromeGarima SrivastavaPas encore d'évaluation
- Malabsorption SyndromeDocument24 pagesMalabsorption SyndromeAswathy ganeshPas encore d'évaluation
- رابعDocument67 pagesرابععلي عليPas encore d'évaluation
- GIT 2021 Lect17Document49 pagesGIT 2021 Lect17Nikkole PhalulaPas encore d'évaluation
- Gallbladder Disease and Its Management-1Document39 pagesGallbladder Disease and Its Management-1adamu mohammadPas encore d'évaluation
- Causes and Diagnosis of SteatorrheaDocument43 pagesCauses and Diagnosis of SteatorrheaJohnRobynDiezPas encore d'évaluation
- 2-Liver DiseasesDocument28 pages2-Liver DiseasesAhmed IsmaillPas encore d'évaluation
- Gastrointestinal Bleeding Causes, Symptoms and TreatmentDocument84 pagesGastrointestinal Bleeding Causes, Symptoms and TreatmentAngela Kristiana IntanPas encore d'évaluation
- DIARRHEA Final Group 8Document65 pagesDIARRHEA Final Group 8angela marie abadillaPas encore d'évaluation
- Miscellaneous SI Disoders, SI TumorsDocument25 pagesMiscellaneous SI Disoders, SI TumorsRanj B. AshrafPas encore d'évaluation
- Lesson 15 Fecalysis and Gastric AnalysisDocument39 pagesLesson 15 Fecalysis and Gastric AnalysisFaith TambongPas encore d'évaluation
- Chronic Diarrhea and Malabsorption GuideDocument50 pagesChronic Diarrhea and Malabsorption GuideIPNATC NEPAL100% (1)
- Malabsorption Syndrome: Causes, Symptoms and TreatmentDocument21 pagesMalabsorption Syndrome: Causes, Symptoms and TreatmentThenmozhi SivajiPas encore d'évaluation
- Hepatomegaly PDFDocument9 pagesHepatomegaly PDFKhadija IbrahimPas encore d'évaluation
- Differential Diagnosis of JaundiceDocument4 pagesDifferential Diagnosis of JaundiceVirag PatilPas encore d'évaluation
- Gall Bladder Diseases by - DR Arun Aggarwal GastroenterologistDocument53 pagesGall Bladder Diseases by - DR Arun Aggarwal GastroenterologistDr. Arun Aggarwal GastroenterologistPas encore d'évaluation
- Fecalysis: Verian John Hoo - Sudario College of Medical TechnologyDocument58 pagesFecalysis: Verian John Hoo - Sudario College of Medical Technologyepson printerPas encore d'évaluation
- 5. Chronic pancreatitis. СholelithiasisDocument58 pages5. Chronic pancreatitis. Сholelithiasischai rinPas encore d'évaluation
- Malabsorption: Causes, Symptoms, and TreatmentDocument75 pagesMalabsorption: Causes, Symptoms, and TreatmentLaith Al TamimiPas encore d'évaluation
- Physiology of Digestion 10-01-2019 PhysiologyDocument29 pagesPhysiology of Digestion 10-01-2019 Physiologysamiul samiPas encore d'évaluation
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesD'EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesPas encore d'évaluation
- Cushing's SyndromeDocument4 pagesCushing's SyndromeVytheeshwaran VedagiriPas encore d'évaluation
- Copper Deficiency AnemiaDocument4 pagesCopper Deficiency AnemiaVytheeshwaran VedagiriPas encore d'évaluation
- KS3 TestDocument6 pagesKS3 TestVytheeshwaran Vedagiri80% (5)
- Key Stage III Biology Question PaperDocument6 pagesKey Stage III Biology Question PaperVytheeshwaran VedagiriPas encore d'évaluation
- Type II HypersensitivityDocument8 pagesType II HypersensitivityVytheeshwaran VedagiriPas encore d'évaluation
- Island Bio GeographyDocument2 pagesIsland Bio GeographyVytheeshwaran VedagiriPas encore d'évaluation
- Hormones SummaryDocument3 pagesHormones SummaryVytheeshwaran VedagiriPas encore d'évaluation
- Adrenocortical InsufficiencyDocument5 pagesAdrenocortical InsufficiencyVytheeshwaran VedagiriPas encore d'évaluation
- A Level Organic Chemistry Mini TestDocument2 pagesA Level Organic Chemistry Mini TestVytheeshwaran VedagiriPas encore d'évaluation
- Introduction To EnzymesDocument43 pagesIntroduction To EnzymesVytheeshwaran Vedagiri100% (2)
- Dispersal and Fair TestDocument3 pagesDispersal and Fair TestVytheeshwaran VedagiriPas encore d'évaluation
- GCSE Lower Tier Chemistry TestDocument5 pagesGCSE Lower Tier Chemistry TestVytheeshwaran VedagiriPas encore d'évaluation
- LAMARCKISM - Rejected Fixity Proposed ADocument2 pagesLAMARCKISM - Rejected Fixity Proposed AVytheeshwaran VedagiriPas encore d'évaluation
- LAMARCKISM - Rejected Fixity Proposed ADocument2 pagesLAMARCKISM - Rejected Fixity Proposed AVytheeshwaran VedagiriPas encore d'évaluation
- Candidate GI HormonesDocument2 pagesCandidate GI HormonesVytheeshwaran Vedagiri100% (2)
- Energetics TestDocument3 pagesEnergetics TestVytheeshwaran Vedagiri100% (1)
- Clinical Enzymology: V. VytheeshwaranDocument40 pagesClinical Enzymology: V. VytheeshwaranVytheeshwaran Vedagiri100% (4)
- Minitest in Formula and EquationsDocument2 pagesMinitest in Formula and EquationsVytheeshwaran VedagiriPas encore d'évaluation
- Metabolism inDocument1 pageMetabolism inVytheeshwaran VedagiriPas encore d'évaluation
- Ventricles of The Brain and CSFDocument22 pagesVentricles of The Brain and CSFVytheeshwaran Vedagiri100% (9)
- Viruses & BacteriophagesDocument3 pagesViruses & BacteriophagesVytheeshwaran Vedagiri100% (7)
- Diabetes MellitusDocument60 pagesDiabetes MellitusVytheeshwaran Vedagiri96% (26)
- Interesting Q&A in Immunology - Part IIIDocument21 pagesInteresting Q&A in Immunology - Part IIIVytheeshwaran Vedagiri100% (14)
- Nucleus - Morphology and FunctionsDocument25 pagesNucleus - Morphology and FunctionsVytheeshwaran Vedagiri96% (24)
- Unconditional Love of A MotherDocument3 pagesUnconditional Love of A MotherVytheeshwaran Vedagiri100% (11)
- Golden Words of Sri RamakrishnaDocument3 pagesGolden Words of Sri RamakrishnaVytheeshwaran Vedagiri100% (13)
- Bacterial GrowthDocument5 pagesBacterial GrowthVytheeshwaran Vedagiri100% (20)
- Interesting Q&A in Immunology - Part IIDocument26 pagesInteresting Q&A in Immunology - Part IIVytheeshwaran Vedagiri90% (10)
- Interesting Q&A in Immunology - Part IDocument24 pagesInteresting Q&A in Immunology - Part IVytheeshwaran Vedagiri100% (9)
- MCI Screening Test (FMGE) Question Paper - 2002Document678 pagesMCI Screening Test (FMGE) Question Paper - 2002Anbu Anbazhagan100% (1)
- LPR by Dr. SS NayyarDocument45 pagesLPR by Dr. SS NayyarSuprit Sn100% (1)
- Balance Retraining YardleyDocument10 pagesBalance Retraining YardleystepwiseclichePas encore d'évaluation
- Wa0012.Document19 pagesWa0012.sg carPas encore d'évaluation
- The Facts About AidsDocument5 pagesThe Facts About AidsTAMBAKI EDMONDPas encore d'évaluation
- Glaucoma 2003Document24 pagesGlaucoma 2003Aryu-hanafiey BoyzzsPas encore d'évaluation
- Development of Cinnamon Oil Based Topical Formulations for their Antibacterial ActivityDocument17 pagesDevelopment of Cinnamon Oil Based Topical Formulations for their Antibacterial ActivityKristen TeePas encore d'évaluation
- Case Investigation Form Coronavirus Disease (COVID-19) : (Check All That Apply, Refer To Appendix 2)Document4 pagesCase Investigation Form Coronavirus Disease (COVID-19) : (Check All That Apply, Refer To Appendix 2)john dave rougel ManzanoPas encore d'évaluation
- Dr. D.N. Prastowo, SP - PD: Bagian Penyakit Dalam Rs. Hana Charitas - Arga Makmur Bengkulu 2017Document45 pagesDr. D.N. Prastowo, SP - PD: Bagian Penyakit Dalam Rs. Hana Charitas - Arga Makmur Bengkulu 2017nanikPas encore d'évaluation
- Cardiovascular DisorderDocument6 pagesCardiovascular DisorderClara De GuzmanPas encore d'évaluation
- Chapter 21 DigestionDocument96 pagesChapter 21 DigestionJwnsbdhdPas encore d'évaluation
- Rania Nasir 22667 Human Development Assignment 1Document2 pagesRania Nasir 22667 Human Development Assignment 1Rania NasirPas encore d'évaluation
- Lecture III-1 Laws of Inheritance Patterns of InheritanceDocument18 pagesLecture III-1 Laws of Inheritance Patterns of InheritanceJÜnn BatacPas encore d'évaluation
- GlomerulonephritisDocument35 pagesGlomerulonephritisapi-19916399Pas encore d'évaluation
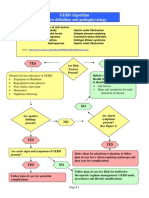
- GERD Algorithm Review Definition and Pathophysiology: NO YESDocument3 pagesGERD Algorithm Review Definition and Pathophysiology: NO YESdianyPas encore d'évaluation
- Nursing Assessment and Interventions for Episiotomy Wound CareDocument2 pagesNursing Assessment and Interventions for Episiotomy Wound Carenethcecilia90% (10)
- Could Neurological Illness Have Infuenced Goyas Pictorial StyleDocument9 pagesCould Neurological Illness Have Infuenced Goyas Pictorial StyleHudson AlieePas encore d'évaluation
- Tuberculosis in Pregnancy Effects Risks TreatmentDocument36 pagesTuberculosis in Pregnancy Effects Risks TreatmentOfel Santillan100% (1)
- Argente v. West Coast Life InsuranceDocument2 pagesArgente v. West Coast Life InsuranceJellyn100% (1)
- Friedreich's Ataxia: Anatomical Structures AffectedDocument26 pagesFriedreich's Ataxia: Anatomical Structures AffectedAparna RawatPas encore d'évaluation
- Fixed Drug EruptionsDocument6 pagesFixed Drug EruptionsArif OktavianPas encore d'évaluation
- Neurological Disorders Key NotesDocument31 pagesNeurological Disorders Key NotesHannah aswiniPas encore d'évaluation
- Curriculum Map in Mapeh 8 (Quarter 3)Document17 pagesCurriculum Map in Mapeh 8 (Quarter 3)Lucelyn Lugas CapoyPas encore d'évaluation
- Women's Heart HealthDocument3 pagesWomen's Heart HealthMatt ThielkePas encore d'évaluation
- An Essay On Yoga and HealthDocument2 pagesAn Essay On Yoga and HealthGentleStrength100% (1)
- BASIC NUTRITION GUIDELINESDocument7 pagesBASIC NUTRITION GUIDELINESMicko QuintoPas encore d'évaluation
- Fluid & Electrolytes Management (Nabil)Document78 pagesFluid & Electrolytes Management (Nabil)Ahmad Nabil Md RosliPas encore d'évaluation
- Burnout Syndrome - Stress in Health Care Professionals Working To Fight Covid-19 in Public HospitalsDocument14 pagesBurnout Syndrome - Stress in Health Care Professionals Working To Fight Covid-19 in Public HospitalsIJAERS JOURNALPas encore d'évaluation
- IMCIDocument11 pagesIMCIJoshua Villarba100% (1)
- AUBF QUiZDocument12 pagesAUBF QUiZGene Narune GaronitaPas encore d'évaluation