Vous aimerez peut-être aussi
- Cricut Cheat Sheet by Alpha - Updated May 2010Document71 pagesCricut Cheat Sheet by Alpha - Updated May 2010Pamm67% (6)
- Parent Intake Interview FormDocument8 pagesParent Intake Interview FormVanessa EstradaPas encore d'évaluation
- Child or Adolescent Client FormsDocument7 pagesChild or Adolescent Client FormsSodfa EttafakshiPas encore d'évaluation
- Case History RecordDocument6 pagesCase History RecordGheylhu AmorPas encore d'évaluation
- Developmental History Form 2016Document5 pagesDevelopmental History Form 2016Mariya KhanPas encore d'évaluation
- Developmental History QuestionnaireDocument6 pagesDevelopmental History QuestionnaireMariana RzPas encore d'évaluation
- Pediatric History FormDocument2 pagesPediatric History FormJim Jose AntonyPas encore d'évaluation
- Adolescent Biopsychosocial AssessmentDocument10 pagesAdolescent Biopsychosocial AssessmentFar Sultan100% (2)
- Journal Baby PDFDocument18 pagesJournal Baby PDFAruni AzizahPas encore d'évaluation
- Stages of Psychosexual DevelopmentDocument2 pagesStages of Psychosexual DevelopmentБексултан Султанов АсановичPas encore d'évaluation
- Child & Adolescent Intake QuestionnaireDocument15 pagesChild & Adolescent Intake QuestionnaireSadar Psychological and Sports Center100% (2)
- Pediatric Assesment FormDocument6 pagesPediatric Assesment FormJenPas encore d'évaluation
- Theories Human DevelopmentDocument37 pagesTheories Human DevelopmentEdgar Alan Poe92% (13)
- Pahintulot para Sa Day Care ServiceDocument9 pagesPahintulot para Sa Day Care ServiceKathleen Rose LibedPas encore d'évaluation
- Nursing Care Health Assessment FormDocument5 pagesNursing Care Health Assessment FormMelanie Bagasol SisonPas encore d'évaluation
- Feeding PDF Feeding History QuesDocument8 pagesFeeding PDF Feeding History QuesSophia DaniilPas encore d'évaluation
- Nov MainDocument148 pagesNov MainPamm100% (1)
- Em3 BabyDocument1 pageEm3 BabyPammPas encore d'évaluation
- Em1 BabyDocument1 pageEm1 BabyPammPas encore d'évaluation
- Management of Low Birth Weight BabiesDocument59 pagesManagement of Low Birth Weight BabiesKiran Khasa100% (2)
- CHN Community Survey FormDocument2 pagesCHN Community Survey FormRamyaj Odagor100% (1)
- Child Case History Form CASDocument5 pagesChild Case History Form CASNoor KhalilPas encore d'évaluation
- Leetaloo Pediatric Therapy: General InformationDocument7 pagesLeetaloo Pediatric Therapy: General InformationrabiyaPas encore d'évaluation
- Case History FormDocument5 pagesCase History Formma jennifer liberoPas encore d'évaluation
- New Patient RegistrationDocument2 pagesNew Patient Registrationnaveenmi2100% (1)
- Ms 2083 EngDocument1 pageMs 2083 Engapi-509258857Pas encore d'évaluation
- Nutritional Clinical History Pregnant WomanDocument13 pagesNutritional Clinical History Pregnant WomanScribdTranslationsPas encore d'évaluation
- Newborn-Infirmation SheetDocument7 pagesNewborn-Infirmation SheetJONABELL B YLAGANPas encore d'évaluation
- Child Health and Development QuestionnaireDocument2 pagesChild Health and Development QuestionnaireFrom Accelerated Derrick SmithPas encore d'évaluation
- Registration For ChildcareDocument2 pagesRegistration For Childcareapi-315547754Pas encore d'évaluation
- Field Trip Permission SlipDocument1 pageField Trip Permission Slipapi-272734430Pas encore d'évaluation
- Nutrition Assessment Questionnaire: Please Bring This Form Completed To Your First AppointmentDocument8 pagesNutrition Assessment Questionnaire: Please Bring This Form Completed To Your First AppointmentNoemiKissPas encore d'évaluation
- Registration Forms 2024Document2 pagesRegistration Forms 2024api-276553863Pas encore d'évaluation
- New Client Questionnaire 12-28-2011Document7 pagesNew Client Questionnaire 12-28-2011api-234610379Pas encore d'évaluation
- Registration PacketDocument8 pagesRegistration PacketTeriElmoreWilsonPas encore d'évaluation
- Junior Tours Medical ReleaseDocument1 pageJunior Tours Medical Releaseapi-235166650Pas encore d'évaluation
- GettingtoknowyourinfantDocument1 pageGettingtoknowyourinfantJessica TaishaPas encore d'évaluation
- NEW OB RISK NICU CASE STUDY FORMAT For 2nd YearDocument16 pagesNEW OB RISK NICU CASE STUDY FORMAT For 2nd YearDrex CuritanaPas encore d'évaluation
- Nurture and Grow Child Development CenterDocument18 pagesNurture and Grow Child Development Centerapi-734701585Pas encore d'évaluation
- Pediatric History TemplateDocument6 pagesPediatric History TemplateseroshPas encore d'évaluation
- ChildenrollmentpapersDocument7 pagesChildenrollmentpapersapi-531837774Pas encore d'évaluation
- Demographic QuestionsDocument6 pagesDemographic QuestionsCynthia Ann Stephanie SapladPas encore d'évaluation
- Enrollment PacketDocument6 pagesEnrollment Packetapi-382256148Pas encore d'évaluation
- Child Background InformationDocument6 pagesChild Background InformationAminath Maana Ibrahim ShakeePas encore d'évaluation
- Medical FormDocument1 pageMedical Formapi-144496227Pas encore d'évaluation
- Adolescent in Take Parent FormDocument4 pagesAdolescent in Take Parent FormEkaterina TrnblPas encore d'évaluation
- AH Form ChildrenDocument11 pagesAH Form ChildrenJosephPas encore d'évaluation
- Medical QuestionnaireDocument10 pagesMedical QuestionnairejibranqqPas encore d'évaluation
- Health History Assessment ToolDocument3 pagesHealth History Assessment ToolDaniela Suarez NimPas encore d'évaluation
- Patient InformationDocument10 pagesPatient InformationFatimahPas encore d'évaluation
- Child Intake2017Document5 pagesChild Intake2017api-358418536Pas encore d'évaluation
- Initial Case History FormDocument3 pagesInitial Case History Formapi-245579214Pas encore d'évaluation
- Health History Form - RJHDocument3 pagesHealth History Form - RJHapi-270094144Pas encore d'évaluation
- FORM B - Physical - STUDENTDocument4 pagesFORM B - Physical - STUDENTJane PPas encore d'évaluation
- DSSC Intake QuestionnaireDocument7 pagesDSSC Intake QuestionnairePrima Hari NastitiPas encore d'évaluation
- Family Health Assessment FormDocument12 pagesFamily Health Assessment Formshandy kyle barbadilloPas encore d'évaluation
- Enrollment PacketDocument3 pagesEnrollment Packetapi-741820810Pas encore d'évaluation
- Admission RecordDocument5 pagesAdmission RecordDeepak SelaPas encore d'évaluation
- Orthopedic and Health History FormsDocument5 pagesOrthopedic and Health History FormstamikanjiPas encore d'évaluation
- Confidential Parent Occupational Physical Therapy 01 15Document7 pagesConfidential Parent Occupational Physical Therapy 01 15Giselle Pezoa WattsonPas encore d'évaluation
- Chnursing NotesDocument21 pagesChnursing Notesjimmy boy canlas jrPas encore d'évaluation
- Hanley Sleep WBK (No Compl) - 12 - 14Document8 pagesHanley Sleep WBK (No Compl) - 12 - 14LufalcoPas encore d'évaluation
- Student MedicalDocument1 pageStudent MedicalbbruntPas encore d'évaluation
- Student Information Sheet 2Document2 pagesStudent Information Sheet 2jhon jhon millarePas encore d'évaluation
- St. George AppDocument9 pagesSt. George AppFutureDDSPas encore d'évaluation
- Application Form Health Examination Form Parents Consent FormDocument1 pageApplication Form Health Examination Form Parents Consent Formapril rose catainaPas encore d'évaluation
- PHAgreementDocument1 pagePHAgreementPammPas encore d'évaluation
- Childrens BiographyDocument3 pagesChildrens BiographyDamaris Pandora SongcalPas encore d'évaluation
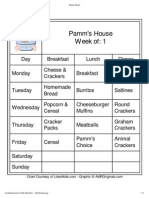
- Pamm's House Week Of: 1: 6/23/2010 Meal ChartDocument1 pagePamm's House Week Of: 1: 6/23/2010 Meal ChartPammPas encore d'évaluation
- AZ Request Exempt Immun Child CareDocument1 pageAZ Request Exempt Immun Child CareDonnaPas encore d'évaluation
- AgreementDocument1 pageAgreementPammPas encore d'évaluation
- PDF Created With Pdffactory Pro Trial VersionDocument2 pagesPDF Created With Pdffactory Pro Trial VersionPamm100% (1)
- Em2 BabyDocument1 pageEm2 BabyPammPas encore d'évaluation
- PDF Created With Pdffactory Pro Trial VersionDocument1 pagePDF Created With Pdffactory Pro Trial VersionPammPas encore d'évaluation
- Sign Language 3Document1 pageSign Language 3PammPas encore d'évaluation
- Sign Language 1Document1 pageSign Language 1PammPas encore d'évaluation
- Sign Language 2Document1 pageSign Language 2PammPas encore d'évaluation
- Esl2 BabyDocument1 pageEsl2 BabyPammPas encore d'évaluation
- Esl4 BabyDocument1 pageEsl4 BabyPammPas encore d'évaluation
- Em4 BabyDocument1 pageEm4 BabyPammPas encore d'évaluation
- E-Health Agenda 4 Stuffed AnimalsDocument1 pageE-Health Agenda 4 Stuffed AnimalsPammPas encore d'évaluation
- E9d MayDocument1 pageE9d MayPamm100% (2)
- E8b AprDocument1 pageE8b AprPammPas encore d'évaluation
- E7a MarDocument1 pageE7a MarPamm100% (1)
- E9c MayDocument1 pageE9c MayPammPas encore d'évaluation
- Eh4 BabyDocument1 pageEh4 BabyPammPas encore d'évaluation
- Eh3 BabyDocument1 pageEh3 BabyPammPas encore d'évaluation
- E7c MarDocument1 pageE7c MarPammPas encore d'évaluation
- E8a AprDocument1 pageE8a AprPamm100% (1)
- E9a MayDocument1 pageE9a MayPamm100% (2)
- E9b MayDocument1 pageE9b MayPamm100% (1)
- E6c FebDocument1 pageE6c FebPammPas encore d'évaluation
- Assessment of Attachment Disorder Symptoms in Foster Children: Comparing Diagnostic Assessment ToolsDocument9 pagesAssessment of Attachment Disorder Symptoms in Foster Children: Comparing Diagnostic Assessment ToolsRendy Marlef HuningkorPas encore d'évaluation
- Kinesiotaping in PediatricsDocument248 pagesKinesiotaping in PediatricsAlbert Slasher100% (24)
- PowerpointDocument31 pagesPowerpointJoanne Mae LuceroPas encore d'évaluation
- Activities Performed in An Infant Welfare ClinicDocument2 pagesActivities Performed in An Infant Welfare ClinicEmmanuela Azubugwu100% (2)
- 4 ANO Aula 2 - 1 Bimestre: Língua InglesaDocument20 pages4 ANO Aula 2 - 1 Bimestre: Língua InglesaAndre BastosPas encore d'évaluation
- 1314-271 Universal PrekDocument395 pages1314-271 Universal PrekJulian A.Pas encore d'évaluation
- Single Child: My AutobiographyDocument2 pagesSingle Child: My AutobiographyFor DrivePas encore d'évaluation
- Miller & Commons (2010) - The Benefits of Attachment Parenting For Infants and Children A Behavioral Developmental ViewDocument14 pagesMiller & Commons (2010) - The Benefits of Attachment Parenting For Infants and Children A Behavioral Developmental ViewFilipus Riaman Napitu SaragihPas encore d'évaluation
- Father-Child Relationships: Michael E. Lamb Charlie LewisDocument16 pagesFather-Child Relationships: Michael E. Lamb Charlie LewisDiana CortejasPas encore d'évaluation
- Family Law Research PaperDocument14 pagesFamily Law Research Paperdeepak KamatchiPas encore d'évaluation
- Developmental Milestones: Mrs. Juliet B. Batac, RN, Man Online Learning Coordinator (Olc)Document19 pagesDevelopmental Milestones: Mrs. Juliet B. Batac, RN, Man Online Learning Coordinator (Olc)Anthonet AtractivoPas encore d'évaluation
- Y2 Phonics ModuleDocument36 pagesY2 Phonics ModulepusatlatihanstemnknPas encore d'évaluation
- Feeding Infants and ToddlersDocument6 pagesFeeding Infants and ToddlersNedum WilfredPas encore d'évaluation
- CindyDocument4 pagesCindyUsama QayyumPas encore d'évaluation
- APPLICATIONDocument7 pagesAPPLICATIONIan Dante ArcangelesPas encore d'évaluation
- Mandated Reporter FormDocument2 pagesMandated Reporter FormLex TalamoPas encore d'évaluation
- Parent Resource CentersDocument12 pagesParent Resource Centersapi-241173571Pas encore d'évaluation
- Executive Order No. 21-2021 Local Council For The Protection of ChildrenDocument2 pagesExecutive Order No. 21-2021 Local Council For The Protection of ChildrenLyn Tabelisma Ozar100% (2)
- Blood RelDocument2 pagesBlood RelNancy ModiPas encore d'évaluation
- Arnett, Emerging AdulthoodDocument281 pagesArnett, Emerging AdulthoodFrancis GayobaPas encore d'évaluation
- AP Draft Foster Care Guidelines 2019Document118 pagesAP Draft Foster Care Guidelines 2019Sai SantoshPas encore d'évaluation
- Work Immersion: Group 1Document3 pagesWork Immersion: Group 1Jorgie GeulinPas encore d'évaluation
- Sexuality EducationDocument38 pagesSexuality EducationSibusiso Ngamla BhebhePas encore d'évaluation
- Attachment During Infancy and Early ChildhoodDocument1 pageAttachment During Infancy and Early ChildhoodLc RolongPas encore d'évaluation
- Appendix NG Group 2Document9 pagesAppendix NG Group 2Jasmine Aika TolenadaPas encore d'évaluation
- Case Study of A Child Age 6-2Document23 pagesCase Study of A Child Age 6-2api-549353756Pas encore d'évaluation