Vous aimerez peut-être aussi
- Adhesive Restoration of Endodontically Treated TeethD'EverandAdhesive Restoration of Endodontically Treated TeethÉvaluation : 3 sur 5 étoiles3/5 (2)
- A Review On Obturating Materials For Deciduous DentitionDocument7 pagesA Review On Obturating Materials For Deciduous DentitionIJAR JOURNALPas encore d'évaluation
- The Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionD'EverandThe Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionÉvaluation : 4 sur 5 étoiles4/5 (1)
- Obturating Materials Used For Pulpectomy in Primary Teeth A ReviewDocument9 pagesObturating Materials Used For Pulpectomy in Primary Teeth A ReviewMohammed SaeedPas encore d'évaluation
- Perawatan Saluran Akar Gigi Desidui DanDocument14 pagesPerawatan Saluran Akar Gigi Desidui DanPipin HeryantoPas encore d'évaluation
- Obturating Materials For Primary TeethDocument77 pagesObturating Materials For Primary TeethSarath MohanPas encore d'évaluation
- Bioactive Glass Nanoparticles (NovaMin®) For Applications in DentistryDocument6 pagesBioactive Glass Nanoparticles (NovaMin®) For Applications in DentistryIOSRjournalPas encore d'évaluation
- Yesterday's Dentistry: Voices from the British Dental Association Oral History ArchiveD'EverandYesterday's Dentistry: Voices from the British Dental Association Oral History ArchivePas encore d'évaluation
- Tooth Bleaching-A Critical Review of The Biological AspectsDocument14 pagesTooth Bleaching-A Critical Review of The Biological AspectsPriska talithaPas encore d'évaluation
- A Z Pulpotomy Agent Literature ReviewDocument8 pagesA Z Pulpotomy Agent Literature ReviewSparklez Dental clinicPas encore d'évaluation
- Overview of Bleaching TechniquesDocument7 pagesOverview of Bleaching TechniquesAnonymous WtgTCQJdNPas encore d'évaluation
- Aodmr Mishra SK Et AlDocument4 pagesAodmr Mishra SK Et AlAsmita SonawnePas encore d'évaluation
- 20 TH JC - SindhuDocument9 pages20 TH JC - SindhuDadi SindhuPas encore d'évaluation
- Research PaperDocument8 pagesResearch Paperapi-366464825Pas encore d'évaluation
- Biomimetic MaterialsDocument88 pagesBiomimetic MaterialsBhoomika SikriPas encore d'évaluation
- Zhao2022 Article ASprayableSuperhydrophobicDentDocument11 pagesZhao2022 Article ASprayableSuperhydrophobicDentXiaodong LiPas encore d'évaluation
- 1733 11068 1 EdDocument10 pages1733 11068 1 EdalekhyaPas encore d'évaluation
- Application of A Tooth-Surface Coating Material Containing Pre-Reacted Glass-IonomerDocument7 pagesApplication of A Tooth-Surface Coating Material Containing Pre-Reacted Glass-IonomerlaloPas encore d'évaluation
- Wisdom Towards Remineralization, A Literature ReviewDocument5 pagesWisdom Towards Remineralization, A Literature ReviewIJAR JOURNALPas encore d'évaluation
- Review - Dental ClinicsDocument13 pagesReview - Dental ClinicsAndrea UrgilesPas encore d'évaluation
- Investigating The Antimicrobial Activity of Different Root Canal Filling Pastes in Deciduous TeethDocument7 pagesInvestigating The Antimicrobial Activity of Different Root Canal Filling Pastes in Deciduous Teethanindya permatasyafiraPas encore d'évaluation
- Evaluasi Keberhasilan Pengisian Saluran Akar Dengan Sediaan Zinc Oxide Eugenol Dan Campuran Calcium Hydroxide Dengan Pasta IodoformDocument7 pagesEvaluasi Keberhasilan Pengisian Saluran Akar Dengan Sediaan Zinc Oxide Eugenol Dan Campuran Calcium Hydroxide Dengan Pasta IodoformAn Nisaa DejandPas encore d'évaluation
- Definisi: Chong BS. 2017. Harty's Endodontics in Clinical Practice 7 Ed. Elsevier LTDDocument61 pagesDefinisi: Chong BS. 2017. Harty's Endodontics in Clinical Practice 7 Ed. Elsevier LTDtillahPas encore d'évaluation
- Glass Ionomer Endodontic Sealers - A Literature ReviewDocument6 pagesGlass Ionomer Endodontic Sealers - A Literature Reviewea1yd6vnPas encore d'évaluation
- 1975 Heithersay Calcium Hydroxide in The Treatment of Puipless Teeth WithDocument21 pages1975 Heithersay Calcium Hydroxide in The Treatment of Puipless Teeth WithJeremy FichauxPas encore d'évaluation
- 10 4 2013Document49 pages10 4 2013Anonymous 2h5lIePas encore d'évaluation
- Discoloration Potential of Endodontic Sealers: A Brief ReviewDocument5 pagesDiscoloration Potential of Endodontic Sealers: A Brief ReviewzaheerbdsPas encore d'évaluation
- Ozone: A New Face of Dentistry: January 2009Document12 pagesOzone: A New Face of Dentistry: January 2009José Antonio López MaldonadoPas encore d'évaluation
- T B - C R B A: Ooth Leaching A Ritical Eview of The Iological SpectsDocument13 pagesT B - C R B A: Ooth Leaching A Ritical Eview of The Iological SpectsalumeraPas encore d'évaluation
- Anderson 1999Document4 pagesAnderson 1999Maria Eduarda de Oliveira Pereira CardosoPas encore d'évaluation
- 5.pulpotomy Medicaments Used in Deciduous Dentition An UpdateDocument18 pages5.pulpotomy Medicaments Used in Deciduous Dentition An UpdateRahma IskPas encore d'évaluation
- 63 Vol. 10 Issue 3 Mar 2019 IJPSR RA 10588Document6 pages63 Vol. 10 Issue 3 Mar 2019 IJPSR RA 10588Dr. Anil LandgePas encore d'évaluation
- Int Endodontic J - 2011 - MohammadiDocument34 pagesInt Endodontic J - 2011 - Mohammadifelipe martinezPas encore d'évaluation
- Bleaching3 Konser2Document3 pagesBleaching3 Konser2akmalsatibiPas encore d'évaluation
- Properties of Calcihydroxide in TicDocument34 pagesProperties of Calcihydroxide in TicPhạm CườngPas encore d'évaluation
- Calcium HydruDocument35 pagesCalcium HydruJayanth KumarPas encore d'évaluation
- Complex Crown Fracture Presenting 5 Hours Post Trauma in A General Dental PracticeDocument8 pagesComplex Crown Fracture Presenting 5 Hours Post Trauma in A General Dental PracticeKamel ArgoubiPas encore d'évaluation
- Stain Removing and Whitening by Baking Soda Dentifrice PDFDocument7 pagesStain Removing and Whitening by Baking Soda Dentifrice PDFDoruPas encore d'évaluation
- Critical Reviews in Oral Biology & Medicine: A Critical Review of The Biological Aspects Tooth BleachingDocument14 pagesCritical Reviews in Oral Biology & Medicine: A Critical Review of The Biological Aspects Tooth BleachingAditi ChandraPas encore d'évaluation
- Zirconia Dental Implants: A Literature Review: Journal of Oral Implantology June 2011Document11 pagesZirconia Dental Implants: A Literature Review: Journal of Oral Implantology June 2011Seno FauziPas encore d'évaluation
- Current Status of Tooth Whitening - Literature Review - Dentistry TodayDocument10 pagesCurrent Status of Tooth Whitening - Literature Review - Dentistry TodayAshbirZammeriPas encore d'évaluation
- Dr. Vibha Hegde - 18Document5 pagesDr. Vibha Hegde - 18Biswaroop ChandraPas encore d'évaluation
- Sintha Nug,+2.+bambang-1Document6 pagesSintha Nug,+2.+bambang-1Rully KasimPas encore d'évaluation
- Efficacy Test of A Toothpaste in Reducing Extrinsic Dental StainDocument7 pagesEfficacy Test of A Toothpaste in Reducing Extrinsic Dental StainJuwita Ratna IntanPas encore d'évaluation
- Bleaching: Bleaching and Its Relevance To Esthetic DentistryDocument64 pagesBleaching: Bleaching and Its Relevance To Esthetic DentistryValentina BadiuPas encore d'évaluation
- 11-Treatment of Immature Permanent Teeth With Pulpal NecrosisDocument5 pages11-Treatment of Immature Permanent Teeth With Pulpal NecrosisAhmed AbdPas encore d'évaluation
- Minimal-Invasive Methods of Cavity Preparation: ISSN 2515-8260 Volume 07, Issue 03, 2020Document11 pagesMinimal-Invasive Methods of Cavity Preparation: ISSN 2515-8260 Volume 07, Issue 03, 2020GowriPas encore d'évaluation
- Obturating Materials in Pediatric Dentistry A ReviDocument9 pagesObturating Materials in Pediatric Dentistry A Revikathuriayug5Pas encore d'évaluation
- Topical Application of Fluoride and Its Anti-Cariogenic EffectDocument7 pagesTopical Application of Fluoride and Its Anti-Cariogenic Effectsintia saputraPas encore d'évaluation
- ImplacleanDocument4 pagesImplacleanbekirarik95Pas encore d'évaluation
- Advanced Drug Delivery Systems For Local Treatment of The Oral CavityDocument24 pagesAdvanced Drug Delivery Systems For Local Treatment of The Oral CavityanjaPas encore d'évaluation
- Intracanal Medicaments in Paediatric EndodonticsDocument5 pagesIntracanal Medicaments in Paediatric EndodonticsJanice EstaPas encore d'évaluation
- The Following Resources Related To This Article Are Available Online atDocument10 pagesThe Following Resources Related To This Article Are Available Online atVerghese George MPas encore d'évaluation
- Evaluation of Three Different Bleaching Agents in Permanent and Primary Teeth: An in Vitro StudyDocument6 pagesEvaluation of Three Different Bleaching Agents in Permanent and Primary Teeth: An in Vitro StudyNadhilahPas encore d'évaluation
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument19 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistselPas encore d'évaluation
- 1 s2.0 S000281771730822X MainDocument3 pages1 s2.0 S000281771730822X MainHoàng Gia Bảo NguyễnPas encore d'évaluation
- Effects of Irrigation Solutions and Calcium Hydroxide Dressing On Root Canal Treatments of Periapical LesionsDocument1 pageEffects of Irrigation Solutions and Calcium Hydroxide Dressing On Root Canal Treatments of Periapical LesionscilapuikoaPas encore d'évaluation
- Rydlyme: The Solution To Your Water Scale ProblemsDocument4 pagesRydlyme: The Solution To Your Water Scale Problemswq3erwqerwerPas encore d'évaluation
- Lysol Brand III Disinfectant All Purpose Cleaner 4 in 1 US EnglishDocument7 pagesLysol Brand III Disinfectant All Purpose Cleaner 4 in 1 US EnglishpatelpiyushbPas encore d'évaluation
- Unidad 6 Orificios. Vertederos Y Resalto HidráulicoDocument5 pagesUnidad 6 Orificios. Vertederos Y Resalto HidráulicoPascual JhonnPas encore d'évaluation
- 170 Gtaw&Smaw Zug Asme (Afri S 5g) WPQDocument4 pages170 Gtaw&Smaw Zug Asme (Afri S 5g) WPQMuhammad Fitransyah Syamsuar PutraPas encore d'évaluation
- Fatty AlcoolDocument16 pagesFatty AlcoolAnamaria UrsuPas encore d'évaluation
- Ni 1882Document81 pagesNi 1882estradeiroPas encore d'évaluation
- Chapter Three: Engine CyclesDocument45 pagesChapter Three: Engine Cyclesapeff97Pas encore d'évaluation
- Etp ManualDocument35 pagesEtp ManualAtul Sharma100% (3)
- Concrete TestingDocument32 pagesConcrete TestingAveesh singh100% (1)
- EMEA - Summary of The Product CharacteristicsDocument20 pagesEMEA - Summary of The Product CharacteristicskadecPas encore d'évaluation
- Sellos HalliteDocument2 pagesSellos HalliteArquimedes PerezPas encore d'évaluation
- Shear Friction MattockDocument10 pagesShear Friction MattockSisina Anish100% (1)
- Alccocrete (HS)Document2 pagesAlccocrete (HS)Siddhesh Kamat MhamaiPas encore d'évaluation
- Spider SilkDocument5 pagesSpider SilkimranPas encore d'évaluation
- Hysteretic Relative Permeability EffectsDocument8 pagesHysteretic Relative Permeability Effectshfdshy12Pas encore d'évaluation
- E11 EsasDocument7 pagesE11 EsasMarche SebastianPas encore d'évaluation
- SDS PAGE Troubleshooting GuideDocument12 pagesSDS PAGE Troubleshooting GuideBhavik ThakarPas encore d'évaluation
- 2017 Batch - UG - Nov - 2019Document29 pages2017 Batch - UG - Nov - 2019sathishPas encore d'évaluation
- Clay TilesDocument5 pagesClay Tilesprashmce100% (1)
- Wiper Seal Data Sheet A02 B 11782 1 enDocument2 pagesWiper Seal Data Sheet A02 B 11782 1 enghanPas encore d'évaluation
- Behavior of Steel Under TensionDocument6 pagesBehavior of Steel Under TensionAshPas encore d'évaluation
- IMUNOMOD TataneasaDocument6 pagesIMUNOMOD TataneasaminunatPas encore d'évaluation
- 2017 Gas Lift CatalogDocument28 pages2017 Gas Lift CatalogHìnhxămNơigóckhuấtTimAnhPas encore d'évaluation
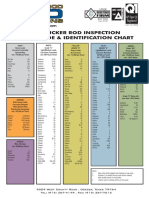
- Permian Rod Operations - Sucker Rod Identification Chart PDFDocument1 pagePermian Rod Operations - Sucker Rod Identification Chart PDFMinimaxou78Pas encore d'évaluation
- (1967) History of The Lenz-Ising ModelDocument13 pages(1967) History of The Lenz-Ising ModelJakler NichelePas encore d'évaluation
- Deflection On The Cantilever BeamDocument11 pagesDeflection On The Cantilever BeamArif AzizAnPas encore d'évaluation
- Mod 7 23-09-09 Extras PDFDocument23 pagesMod 7 23-09-09 Extras PDFU TubePas encore d'évaluation
- Titration of Sodium Hydroxide With Hydrochloric AcidDocument3 pagesTitration of Sodium Hydroxide With Hydrochloric AcidMir HashemiPas encore d'évaluation
- Microwave Level SwitchDocument3 pagesMicrowave Level SwitchDidinAndresIIPas encore d'évaluation
- Nanomaterials A Danger or A Promise?Document398 pagesNanomaterials A Danger or A Promise?Criseida RuizPas encore d'évaluation