Vous aimerez peut-être aussi
- Heather Spencer Police ReportDocument31 pagesHeather Spencer Police Reportthe kingfish0% (1)
- Hayashi Reiki ManualDocument14 pagesHayashi Reiki Manualboomerb100% (4)
- Paramedic Assist Course OutlineDocument6 pagesParamedic Assist Course Outlinedandude505Pas encore d'évaluation
- BATESDocument9 pagesBATESSheryhan BaylePas encore d'évaluation
- Psychiatric Assessment and Evaluation: History TakingDocument9 pagesPsychiatric Assessment and Evaluation: History TakingWaheedullah AhmadiPas encore d'évaluation
- 13 Areas of AssessmentDocument3 pages13 Areas of AssessmentSoleil MaxwellPas encore d'évaluation
- 4.10.17final Clinical Trials Talk.4.10.2017 - 300526 - 284 - 30426 - v1Document67 pages4.10.17final Clinical Trials Talk.4.10.2017 - 300526 - 284 - 30426 - v1Mohammed HammedPas encore d'évaluation
- Psychological DisordersDocument21 pagesPsychological DisordersMark100% (2)
- Meaney Caitlin RN ResumeDocument2 pagesMeaney Caitlin RN Resumeapi-384247457Pas encore d'évaluation
- AmbSpecs KKK 1822Document110 pagesAmbSpecs KKK 1822philcogabiPas encore d'évaluation
- Case Investigation Forms - Pidsrmop3ed 1Document16 pagesCase Investigation Forms - Pidsrmop3ed 1RHU Dupax del Sur100% (3)
- NCP For RDSDocument3 pagesNCP For RDSKevin P. Feliciano74% (23)
- 1 - Mattu, Amal ECGsDocument68 pages1 - Mattu, Amal ECGsKhan A Reh50% (2)
- Kult Character SheetDocument7 pagesKult Character SheetSynder CatPas encore d'évaluation
- 95 EVOC Instructor GuideDocument637 pages95 EVOC Instructor Guidedandude505100% (1)
- Crowns and Other Extra-Coronal RestorationDocument116 pagesCrowns and Other Extra-Coronal RestorationDennis La Torre Zea100% (4)
- Dnb-General Surgery: Competency Based Training ProgrammeDocument49 pagesDnb-General Surgery: Competency Based Training ProgrammeLakshmi Mounica Grandhi100% (1)
- Johns Hopkins PCRDocument1 pageJohns Hopkins PCRdandude505Pas encore d'évaluation
- Comparison of Mean Using Paired-Observations: Two Populations Hypothesis TestingDocument9 pagesComparison of Mean Using Paired-Observations: Two Populations Hypothesis TestingNgoc NguyenPas encore d'évaluation
- LaporanDocument2 pagesLaporanyusviaPas encore d'évaluation
- Contoh LaporanDocument1 pageContoh LaporanyusviaPas encore d'évaluation
- Bản sao 08 - Two Populations Hypothesis TestingDocument9 pagesBản sao 08 - Two Populations Hypothesis TestingPhương AnhhPas encore d'évaluation
- Laporan KesehatanDocument1 pageLaporan KesehatanyusviaPas encore d'évaluation
- R.'lelrnlrl (Ofts:,, " I C L eDocument7 pagesR.'lelrnlrl (Ofts:,, " I C L eKimchiandTofuPas encore d'évaluation
- No. Nama JK Tanggal Lahir Interpretasi Hasil Kesimpulan Saran Bahasa Jumlah Usia (Tahun Dan Bulan) Personal Sosial Motorik Halus Motorik KasarDocument3 pagesNo. Nama JK Tanggal Lahir Interpretasi Hasil Kesimpulan Saran Bahasa Jumlah Usia (Tahun Dan Bulan) Personal Sosial Motorik Halus Motorik KasarMonyet...Pas encore d'évaluation
- Capd 000001119Document2 pagesCapd 000001119Capitol Breach DiscoveryPas encore d'évaluation
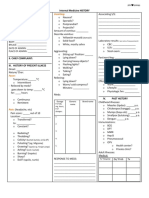
- Internal Medicine HISTORYDocument4 pagesInternal Medicine HISTORYClaire FPas encore d'évaluation
- Hypothetical IE of Spinal Cord Injury (SCI)Document12 pagesHypothetical IE of Spinal Cord Injury (SCI)MIKEE MEDRANOPas encore d'évaluation
- Malliga R. Iyer, Resat Cinar, Nathan J. Coffey, Robert J. Chorvat and George KunosDocument16 pagesMalliga R. Iyer, Resat Cinar, Nathan J. Coffey, Robert J. Chorvat and George KunosJuan RorizPas encore d'évaluation
- Case Study 3 CVD Bleed HCVD Type 2 DM CICD Stage 5 WorksheetDocument27 pagesCase Study 3 CVD Bleed HCVD Type 2 DM CICD Stage 5 WorksheetJade HemmingsPas encore d'évaluation
- Internal Medicine HISTORYDocument4 pagesInternal Medicine HISTORYNorjetalexis CabreraPas encore d'évaluation
- JeromeDocument2 pagesJeromeNads DecapiaPas encore d'évaluation
- Iii. Physical Assessment and Review of SystemDocument7 pagesIii. Physical Assessment and Review of SystemBiya MacuntePas encore d'évaluation
- Acute Flaccid Paralysis: Case Investigation FormDocument2 pagesAcute Flaccid Paralysis: Case Investigation FormPaul Angelo E. Caliva0% (1)
- Insta VocabDocument2 pagesInsta Vocabapi-584574665Pas encore d'évaluation
- LaporanDocument1 pageLaporanyusviaPas encore d'évaluation
- DI Arrhea Part-1 Generali Nformati ON: I NDI VI Dualprofi LEDocument12 pagesDI Arrhea Part-1 Generali Nformati ON: I NDI VI Dualprofi LEsandeepPas encore d'évaluation
- Diabetes insipi-WPS OfficeDocument19 pagesDiabetes insipi-WPS OfficeBharat Singh BanshiwalPas encore d'évaluation
- CRT 7Document8 pagesCRT 7api-643868511Pas encore d'évaluation
- DELSIncident Report FormDocument2 pagesDELSIncident Report FormUnderwaterSciencePas encore d'évaluation
- OME Screening Checklist 1697602735Document2 pagesOME Screening Checklist 1697602735txy2n9pdwqPas encore d'évaluation
- Post Operative CataractDocument1 pagePost Operative CataractFrinkaWijayaPas encore d'évaluation
- LaporanDocument1 pageLaporanyusviaPas encore d'évaluation
- Tutorial Letter 003/0/2021: Statistical Inference IDocument7 pagesTutorial Letter 003/0/2021: Statistical Inference IRegina ThobelaPas encore d'évaluation
- Patient Information: DateDocument8 pagesPatient Information: Datemehdi chahrour100% (1)
- RH Blood Group System 2Document17 pagesRH Blood Group System 2janPas encore d'évaluation
- New Patient PaperworkDocument3 pagesNew Patient PaperworkΒασίλης ΦραγκιαδάκηςPas encore d'évaluation
- Slide Fluid TherapyDocument56 pagesSlide Fluid TherapyanantaPas encore d'évaluation
- Lecture4 PDFDocument46 pagesLecture4 PDFRed KnightPas encore d'évaluation
- Our Lady of Perpetual Help: I. Patient'S Personal InformationDocument10 pagesOur Lady of Perpetual Help: I. Patient'S Personal InformationOkram OrlinaPas encore d'évaluation
- Easy Ukul El e L Esson I N T He Key of D. PL Ay Al Ong Wi T H T Hi S T Ut or I Al (Scan)Document2 pagesEasy Ukul El e L Esson I N T He Key of D. PL Ay Al Ong Wi T H T Hi S T Ut or I Al (Scan)AntonyAntonyPas encore d'évaluation
- Vomiting:: Internal Medicine HISTORY I. Patient'S Profile A. GENERAL DATA (Time: - )Document4 pagesVomiting:: Internal Medicine HISTORY I. Patient'S Profile A. GENERAL DATA (Time: - )Peter GirasolPas encore d'évaluation
- RevisedDocument16 pagesRevisedZymer Lee AbasoloPas encore d'évaluation
- Winning The War in Your Mind PDFdrive - Com.coDocument43 pagesWinning The War in Your Mind PDFdrive - Com.cosipra2438Pas encore d'évaluation
- Hairat 2Document1 pageHairat 2AlhassanPas encore d'évaluation
- T Distribution.Document25 pagesT Distribution.JOMALYN J. NUEVOPas encore d'évaluation
- Adobe Scan 06-Nov-2023Document2 pagesAdobe Scan 06-Nov-2023s k sPas encore d'évaluation
- Inglés para Médicos IIDocument29 pagesInglés para Médicos IICarla JaegerPas encore d'évaluation
- Clinical Data Collection ToolDocument3 pagesClinical Data Collection ToolkatiegracemcleodPas encore d'évaluation
- Encoder Decoder RecordDocument10 pagesEncoder Decoder RecordThanviomPas encore d'évaluation
- Altered Carbon Cast Character SheetsDocument5 pagesAltered Carbon Cast Character SheetsDandier SteelPas encore d'évaluation
- Intake Forms 2020Document5 pagesIntake Forms 2020api-624857223Pas encore d'évaluation
- BellsDocument6 pagesBellsMae NochePas encore d'évaluation
- HA 1st Lecture Health HistoryDocument7 pagesHA 1st Lecture Health HistoryChilled Moo MooPas encore d'évaluation
- All Sheets GMsDocument4 pagesAll Sheets GMsDarknessPas encore d'évaluation
- Q15 Template - Sheet1 PDFDocument1 pageQ15 Template - Sheet1 PDFPreston LeePas encore d'évaluation
- MiningandEngineeringWorld 10676349Document91 pagesMiningandEngineeringWorld 10676349inderjeet SinghPas encore d'évaluation
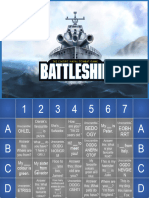
- Battleship - Meeting and GreetingDocument2 pagesBattleship - Meeting and GreetingHilde Reis JuniorPas encore d'évaluation
- I Ngeni Erí Aenprocesosquí Mi CosDocument1 pageI Ngeni Erí Aenprocesosquí Mi CosJuana GomezPas encore d'évaluation
- The Dfferent Ones by Rod SerlingDocument7 pagesThe Dfferent Ones by Rod SerlingArayah FowlerPas encore d'évaluation
- CAMP - Cervical Radic - ColladoDocument5 pagesCAMP - Cervical Radic - ColladoSergi Lee OratePas encore d'évaluation
- MR - Saravanan SID No: NUM 046022:::: Sample Collected and SentDocument1 pageMR - Saravanan SID No: NUM 046022:::: Sample Collected and Sentventhamarai sPas encore d'évaluation
- Dictyostelium Discoideum: A Developmental SystemD'EverandDictyostelium Discoideum: A Developmental SystemÉvaluation : 5 sur 5 étoiles5/5 (1)
- At The Legal Limit - NYTime..Document6 pagesAt The Legal Limit - NYTime..dandude505Pas encore d'évaluation
- Legal Aspects of EMSDocument2 pagesLegal Aspects of EMSdandude505Pas encore d'évaluation
- 1994 Curriculum EmtDocument4 pages1994 Curriculum Emtdandude505Pas encore d'évaluation
- Home Region 1 Committees Education Resources DP1Document1 pageHome Region 1 Committees Education Resources DP1dandude505Pas encore d'évaluation
- AD DeathDocument25 pagesAD Deathdandude505Pas encore d'évaluation
- Mandatory ReportingDocument1 pageMandatory Reportingdandude505Pas encore d'évaluation
- Umass Lowell PCRDocument1 pageUmass Lowell PCRdandude505Pas encore d'évaluation
- Advice For New EMT's - Pink..Document12 pagesAdvice For New EMT's - Pink..dandude505Pas encore d'évaluation
- EMS On-Call Pay and The FLSADocument3 pagesEMS On-Call Pay and The FLSAdandude505Pas encore d'évaluation
- New York State PCRDocument3 pagesNew York State PCRdandude505Pas encore d'évaluation
- New York State FR PCRDocument2 pagesNew York State FR PCRdandude505Pas encore d'évaluation
- Wustl PCRDocument2 pagesWustl PCRdandude505Pas encore d'évaluation
- Mass Event Zone PlanningDocument9 pagesMass Event Zone Planningdandude505Pas encore d'évaluation
- Boston PCRDocument1 pageBoston PCRdandude505Pas encore d'évaluation
- Va Tech Standby ReportDocument1 pageVa Tech Standby Reportdandude505Pas encore d'évaluation
- Va Tech Standby ReleaseDocument2 pagesVa Tech Standby Releasedandude505Pas encore d'évaluation
- New Hampshire PCRDocument2 pagesNew Hampshire PCRdandude505Pas encore d'évaluation
- Rice University's Public Access Defib ProposalDocument13 pagesRice University's Public Access Defib Proposaldandude505Pas encore d'évaluation
- Treatment Protocols 704.JUNE.08Document161 pagesTreatment Protocols 704.JUNE.08dandude505100% (3)
- Virginia PCRDocument3 pagesVirginia PCRdandude505Pas encore d'évaluation
- (J) Jtij: Muhlenberg College EmsDocument3 pages(J) Jtij: Muhlenberg College Emsdandude505Pas encore d'évaluation
- Laws of The House of GodDocument2 pagesLaws of The House of Goddandude505Pas encore d'évaluation
- Continuing Education ManualDocument33 pagesContinuing Education Manualdandude505Pas encore d'évaluation
- Sick Ems HumorDocument13 pagesSick Ems Humordandude505100% (1)
- EmtbnscDocument681 pagesEmtbnscGel OmugtongPas encore d'évaluation
- Sitogenetika Dan Peranannya Dalam Keganasan Hematologi: ResearchDocument23 pagesSitogenetika Dan Peranannya Dalam Keganasan Hematologi: ResearchFebryanti Priskila SilaenPas encore d'évaluation
- Teleradiologi: Cross Reporting & Smart AssignDocument17 pagesTeleradiologi: Cross Reporting & Smart Assignrafael100% (1)
- Jouve FAQ'sDocument3 pagesJouve FAQ'sSamuel A BotPas encore d'évaluation
- Measles and Rubella Global UpdateDocument21 pagesMeasles and Rubella Global UpdateAngga Mariantono EdelweisPas encore d'évaluation
- Pathophysiology QBDocument5 pagesPathophysiology QBVimlesh PalPas encore d'évaluation
- Common Abbrevia-WPS OfficeDocument8 pagesCommon Abbrevia-WPS OfficeChristian Nicolas RabagoPas encore d'évaluation
- Norethisterone JournalDocument29 pagesNorethisterone JournalAditya Syah PutraPas encore d'évaluation
- Aplikasi Terapi Generalis Dalam Pemberian Asuhan Keperawatan Jiwa Pada Nn. R Dengan HalusinasiDocument13 pagesAplikasi Terapi Generalis Dalam Pemberian Asuhan Keperawatan Jiwa Pada Nn. R Dengan Halusinasicindy veronikaPas encore d'évaluation
- Artículo COVID 19 Síntomas Al AñoDocument12 pagesArtículo COVID 19 Síntomas Al AñoSMIBA MedicinaPas encore d'évaluation
- Superficial Corneal Injury and Foreign BodyDocument1 pageSuperficial Corneal Injury and Foreign BodyandinurulpratiwiPas encore d'évaluation
- Dementia - StatPearls - NCBI BookshelfDocument7 pagesDementia - StatPearls - NCBI BookshelfSMA N 1 TOROHPas encore d'évaluation
- Funda Lab - Prelim ReviewerDocument16 pagesFunda Lab - Prelim ReviewerNikoruPas encore d'évaluation
- Desire Carmona - Informe Médico - TRADUCIDODocument3 pagesDesire Carmona - Informe Médico - TRADUCIDONelson FerrerPas encore d'évaluation
- GAD Aos 40 AnosDocument7 pagesGAD Aos 40 AnosrafaelplPas encore d'évaluation
- Physiologic Changes in Pregnancy: 1. UterusDocument14 pagesPhysiologic Changes in Pregnancy: 1. UterusNiña Ricci MtflcoPas encore d'évaluation
- Heavy Menstrual Bleeding Assessment and Management PDF 1837701412549Document33 pagesHeavy Menstrual Bleeding Assessment and Management PDF 1837701412549Meera Al AliPas encore d'évaluation
- IMF Screw Set. For Temporary, Peri Operative Stabilisation of The Occlusion in AdultsDocument12 pagesIMF Screw Set. For Temporary, Peri Operative Stabilisation of The Occlusion in AdultsAnonymous LnWIBo1GPas encore d'évaluation
- Knowledge and Attitudes of Pediatric Clinicians Regarding Pediatric Pain ManagementDocument11 pagesKnowledge and Attitudes of Pediatric Clinicians Regarding Pediatric Pain ManagementIkek StanzaPas encore d'évaluation
- GI TractDocument51 pagesGI TractOktalia Rahmawati RahayuPas encore d'évaluation
- Special Chemistry: Test Name Current Result Previous Result Unit Normal RangeDocument1 pageSpecial Chemistry: Test Name Current Result Previous Result Unit Normal RangeddssPas encore d'évaluation