Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- House Hearing, 111TH Congress - Antibiotic Resistance and The Use of Antibiotics in Animal AgricultureDocument359 pagesHouse Hearing, 111TH Congress - Antibiotic Resistance and The Use of Antibiotics in Animal AgricultureScribd Government DocsPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- NCP Fdar Fin.Document8 pagesNCP Fdar Fin.Bissette DomingoPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Nadi Shodhana (Stage 1)Document3 pagesNadi Shodhana (Stage 1)Béla JózsiPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Growth and Development Orthodontic MCQDocument4 pagesGrowth and Development Orthodontic MCQLamar Mohamed50% (8)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Uwise HYDocument3 pagesUwise HYJack GuccionePas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Most Expected Vocabulary Ebook by Prashant SirDocument35 pagesMost Expected Vocabulary Ebook by Prashant SirPriya GuptaPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Fever With RashDocument89 pagesFever With RashJohna Pauline MandacPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Practical Hematology ManualDocument48 pagesPractical Hematology ManualHaael88Pas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Practice Questions: Respiratory SystemDocument6 pagesPractice Questions: Respiratory SystemTraceyPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Biology M8 Integumentary & Excretory SystemsDocument23 pagesBiology M8 Integumentary & Excretory SystemsDiana Dealino-SabandalPas encore d'évaluation
- Legal Med. Report-QueenDocument61 pagesLegal Med. Report-QueenQuinnee VallejosPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Class 11 Compiled Chintu Notes ..Document76 pagesClass 11 Compiled Chintu Notes ..Mohammed ArifuddinPas encore d'évaluation
- Journal 1Document2 pagesJournal 1Intan KartikasariPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- (Advances in Parasitology, Volume 91) David Rollinson, Russell Stothard-Elsevier - Academic Press (2016)Document430 pages(Advances in Parasitology, Volume 91) David Rollinson, Russell Stothard-Elsevier - Academic Press (2016)Fabián A. Chavez EcosPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Symbiosis Practice PDFDocument10 pagesSymbiosis Practice PDFMark ArcePas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
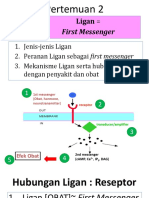
- 2 Ligan First MassengerDocument32 pages2 Ligan First MassengerikhararaPas encore d'évaluation
- Pathophysiology of Cyanotic Congenital Heart DefectsDocument16 pagesPathophysiology of Cyanotic Congenital Heart Defectsbonar46Pas encore d'évaluation
- A Practicle Handbook of Dairy HusbandryDocument122 pagesA Practicle Handbook of Dairy HusbandryGian Niotis100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Supervisi Berjenjang Di Era Pandemi Covid-19 Dalam Manajemen KeperawatanDocument10 pagesSupervisi Berjenjang Di Era Pandemi Covid-19 Dalam Manajemen Keperawatanfebrian rahmatPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- AmenorrheaDocument148 pagesAmenorrheaAbhishek VijayakumarPas encore d'évaluation
- We Are Fungi Ebook Christine NishiyamaDocument23 pagesWe Are Fungi Ebook Christine Nishiyamajeej00Pas encore d'évaluation
- tmpB0AD TMPDocument10 pagestmpB0AD TMPFrontiersPas encore d'évaluation
- Ingested Foreign BodyDocument18 pagesIngested Foreign BodyTeuku FaisalPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Seven Spotted LadybugDocument1 pageSeven Spotted LadybugAlcindorLeadonPas encore d'évaluation
- Host Parasite InteractionDocument20 pagesHost Parasite InteractionRhomizal MazaliPas encore d'évaluation
- Model Test One Structure and Written ExpressionDocument10 pagesModel Test One Structure and Written ExpressionEka KurniatiPas encore d'évaluation
- Kato Thick Kato KatzDocument3 pagesKato Thick Kato KatzジェスPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Ollie The Octopus Only Had Seven 1Document5 pagesOllie The Octopus Only Had Seven 1SuriyantoSpencerPas encore d'évaluation
- 1-1 Animal Vaccine Business Opportunity With CavacDocument34 pages1-1 Animal Vaccine Business Opportunity With CavacFamar HivePas encore d'évaluation
- Eipecs - Eipisi:z) : Vârf, CulmeDocument4 pagesEipecs - Eipisi:z) : Vârf, CulmeAlina CimpeanuPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)