Vous aimerez peut-être aussi
- Anatomy and Physiology DengueDocument5 pagesAnatomy and Physiology Denguenva226Pas encore d'évaluation
- The Difference Between Toxic and Nontoxic GoiterDocument2 pagesThe Difference Between Toxic and Nontoxic GoiterJawad Rehman100% (1)
- Annotated Group 2 Impetigo Concept Mapping 1Document30 pagesAnnotated Group 2 Impetigo Concept Mapping 1DHANE ANN CAMPOSANOPas encore d'évaluation
- Anti HistamineDocument15 pagesAnti HistamineOoi Ah GuanPas encore d'évaluation
- Lecture NCM 109Document11 pagesLecture NCM 109Evangeline Anne MacanasPas encore d'évaluation
- Case StudyDocument21 pagesCase StudyLuige AvilaPas encore d'évaluation
- Addison'sDocument4 pagesAddison'sKoRnflakesPas encore d'évaluation
- Chronic PyelonephritisDocument5 pagesChronic PyelonephritisIsak ShatikaPas encore d'évaluation
- Seizure PathophysiologyDocument2 pagesSeizure PathophysiologyqwertyuiopPas encore d'évaluation
- OTITIS Concept MapDocument7 pagesOTITIS Concept MapEllePas encore d'évaluation
- The Modified Falls Efficacy Scale: Name DateDocument1 pageThe Modified Falls Efficacy Scale: Name Datemaria murcia100% (1)
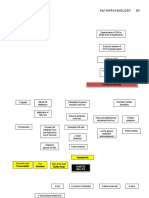
- Pathophy NCADocument1 pagePathophy NCAKaren ValdezPas encore d'évaluation
- Schistosomiasis (From Anatomy To Pathophysiology)Document10 pagesSchistosomiasis (From Anatomy To Pathophysiology)Tiger Knee100% (1)
- Hypothyroidism PathophysiologyDocument1 pageHypothyroidism PathophysiologyCleo Joyce C. CristalPas encore d'évaluation
- HCVD Cad Cva InfarctionDocument2 pagesHCVD Cad Cva InfarctionPamela DomingoPas encore d'évaluation
- Failure of DescentDocument39 pagesFailure of DescentfahlevyPas encore d'évaluation
- BLOOD DYSCRASIA ADocument2 pagesBLOOD DYSCRASIA AMyami Bersamen100% (1)
- TetanusDocument23 pagesTetanusNadya Noor Mulya Putri100% (1)
- Hypokalemia Periodic ParalysisDocument14 pagesHypokalemia Periodic ParalysisJennirose JingPas encore d'évaluation
- Surgical Management For Cryptorchidism With Nursing ManagementsDocument4 pagesSurgical Management For Cryptorchidism With Nursing ManagementsAprille Claire MoralesPas encore d'évaluation
- Cretenism Case StudyDocument8 pagesCretenism Case StudyMonica Marie MoralesPas encore d'évaluation
- Ideal Pathophysiology of Diabetes Mellitus Type IIDocument6 pagesIdeal Pathophysiology of Diabetes Mellitus Type IIAffrida Nurlily Chintya WidariPas encore d'évaluation
- Spina Bifida Concept Map PDFDocument1 pageSpina Bifida Concept Map PDFnot realPas encore d'évaluation
- Case Pres A1-RhdDocument11 pagesCase Pres A1-RhdCharm TanyaPas encore d'évaluation
- Adult HealthDocument28 pagesAdult HealthL1NEDS DPas encore d'évaluation
- COVID-19: Brian, Fernando, Jason, FelitaDocument8 pagesCOVID-19: Brian, Fernando, Jason, FelitaCharson ChenPas encore d'évaluation
- MedSurg Notes - Cancer of The LiverDocument2 pagesMedSurg Notes - Cancer of The LiverMae CeaesarPas encore d'évaluation
- Case Study On Toxic GoiterDocument5 pagesCase Study On Toxic GoiterRein EstradaPas encore d'évaluation
- SuffixesDocument3 pagesSuffixesgrgicosPas encore d'évaluation
- Cancer of The ColonDocument8 pagesCancer of The Colonnot your medz duranPas encore d'évaluation
- Group 2 DkaDocument73 pagesGroup 2 DkaAkio Ozaraga100% (1)
- Gordon's Functional HealthDocument2 pagesGordon's Functional HealthReina ArabellePas encore d'évaluation
- German MeaslesDocument8 pagesGerman MeaslesYdynn Parejas GavinaPas encore d'évaluation
- Abnormal Uterine BleedingDocument2 pagesAbnormal Uterine BleedingNatasha EnidPas encore d'évaluation
- This Study Resource Was: HypomagnesemiaDocument1 pageThis Study Resource Was: HypomagnesemiaMaica LectanaPas encore d'évaluation
- Kaposi's SarcomaDocument6 pagesKaposi's SarcomaveremkovichPas encore d'évaluation
- Pathophysiology of Anxiety DisordersDocument3 pagesPathophysiology of Anxiety DisordersFaizatunnajjah FmzPas encore d'évaluation
- Baby Kiran Aged 7 Years Brought To The Emergency Opd Accomp: ScenarioDocument22 pagesBaby Kiran Aged 7 Years Brought To The Emergency Opd Accomp: ScenariobhavanaPas encore d'évaluation
- Sudden Infant Death SyndromeDocument5 pagesSudden Infant Death SyndromeJanelle Gift SenarloPas encore d'évaluation
- Case 6: Delos Reyes, Lasac, Majid, Mamangun, YuDocument49 pagesCase 6: Delos Reyes, Lasac, Majid, Mamangun, YuAbdullah Bin MajidPas encore d'évaluation
- Module 12Document12 pagesModule 12mirai desuPas encore d'évaluation
- Mechanism of HypertensionDocument4 pagesMechanism of HypertensionAlya Putri KhairaniPas encore d'évaluation
- Nasogastric Tube Feeding ML4763 PDFDocument7 pagesNasogastric Tube Feeding ML4763 PDFStereo PodPas encore d'évaluation
- Pathophysiology Cushing S SyndromeDocument4 pagesPathophysiology Cushing S SyndromeMaria Luisa VillalunaPas encore d'évaluation
- DOH ProgramsDocument6 pagesDOH ProgramsMichael VillavertPas encore d'évaluation
- Pediatric Assesment Tool: Sakit Jud Siya, Mga 8 Siguro."Document5 pagesPediatric Assesment Tool: Sakit Jud Siya, Mga 8 Siguro."RubelleMicahCagampangSapongPas encore d'évaluation
- Diabetes PathoDocument2 pagesDiabetes Pathodrewcel100% (1)
- Urolithiasis PDFDocument4 pagesUrolithiasis PDFaaaPas encore d'évaluation
- Papillary Thyroid Ca: Group. 1 B Grand CaseDocument16 pagesPapillary Thyroid Ca: Group. 1 B Grand CaseAdora Dela CruzPas encore d'évaluation
- Stroke (Bisaya and English)Document4 pagesStroke (Bisaya and English)AnaPas encore d'évaluation
- NCP Risk InfectionDocument1 pageNCP Risk InfectionEni RahmawatiPas encore d'évaluation
- Case Study in KidneyDocument3 pagesCase Study in KidneyVenice VelascoPas encore d'évaluation
- Inflammatory Bowel DiseaseDocument31 pagesInflammatory Bowel DiseaseMuhammad100% (1)
- Pathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsDocument2 pagesPathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsAb Staholic Boii100% (1)
- PBL Copd: 1) Mechanics of RespirationDocument34 pagesPBL Copd: 1) Mechanics of RespirationAhmadPas encore d'évaluation
- Thyroid Lobectomy and IsthmusectomyDocument12 pagesThyroid Lobectomy and IsthmusectomyAgustina100% (1)
- Case (Acute Gastroenteritis) Group 4Document36 pagesCase (Acute Gastroenteritis) Group 4EljhayrosPas encore d'évaluation
- Bệnh Não GanDocument4 pagesBệnh Não GanLinhPas encore d'évaluation
- JTR2014 649502 PDFDocument7 pagesJTR2014 649502 PDFIlmanPas encore d'évaluation
- KQ2H M1 InchDocument5 pagesKQ2H M1 Inch林林爸爸Pas encore d'évaluation
- Structural Tanks and ComponentsDocument19 pagesStructural Tanks and ComponentsRodolfo Olate G.Pas encore d'évaluation
- Evaluation of Bond Strenght of Dentin Adhesive at Dry and Moist Dentin-Resin Interface PDFDocument4 pagesEvaluation of Bond Strenght of Dentin Adhesive at Dry and Moist Dentin-Resin Interface PDFOpris PaulPas encore d'évaluation
- Mechanical Interview Questions and Answers - Fluid MechanicsDocument2 pagesMechanical Interview Questions and Answers - Fluid MechanicsannukiitPas encore d'évaluation
- Azure Essentials: Module 5: Azure Cost Management and Service Level AgreementsDocument9 pagesAzure Essentials: Module 5: Azure Cost Management and Service Level Agreementsrajagopalan19Pas encore d'évaluation
- Flaxseed Paper PublishedDocument4 pagesFlaxseed Paper PublishedValentina GarzonPas encore d'évaluation
- Ear CandlingDocument2 pagesEar CandlingpowerleaderPas encore d'évaluation
- Abrams Clinical Drug Therapy Rationales For Nursing Practice 11th Edition Test BankDocument6 pagesAbrams Clinical Drug Therapy Rationales For Nursing Practice 11th Edition Test BankWilliam Nakken100% (28)
- Brooklyn Hops BreweryDocument24 pagesBrooklyn Hops BrewerynyairsunsetPas encore d'évaluation
- Lab Risk AssessmentDocument8 pagesLab Risk Assessmentaqilah haronPas encore d'évaluation
- Kidney Diet DelightsDocument20 pagesKidney Diet DelightsArturo Treviño MedinaPas encore d'évaluation
- Me22 M1a1Document2 pagesMe22 M1a1Jihoo JungPas encore d'évaluation
- PHC Visit: Chandreswor Primary Health Care Centre: TH TH TH THDocument6 pagesPHC Visit: Chandreswor Primary Health Care Centre: TH TH TH THShashanka PoudelPas encore d'évaluation
- Bakery Business PlanDocument15 pagesBakery Business PlanGayu AishuPas encore d'évaluation
- Parle G ReportDocument7 pagesParle G ReportnikhilPas encore d'évaluation
- Design of Sour Water Stripping System: February 2009Document23 pagesDesign of Sour Water Stripping System: February 2009mohsen ranjbarPas encore d'évaluation
- TMP DEDADocument8 pagesTMP DEDAFrontiersPas encore d'évaluation
- Competency Competency Multiple Choice Multiple Choice ComputationDocument4 pagesCompetency Competency Multiple Choice Multiple Choice ComputationAaron James LicoPas encore d'évaluation
- Science Grade 7: Active Reading Note-Taking GuideDocument140 pagesScience Grade 7: Active Reading Note-Taking Guideurker100% (1)
- CHN REVIEWER LESSON 1 and 2Document9 pagesCHN REVIEWER LESSON 1 and 2Imogen MasumiPas encore d'évaluation
- A-Level: Psychology 7182/1Document20 pagesA-Level: Psychology 7182/1Queen Bee (Tt)Pas encore d'évaluation
- Nama Anggota: Dede Wiyanto Endri Murni Hati Rukhi Hasibah Tugas: Bahasa Inggris (Narrative Text)Document3 pagesNama Anggota: Dede Wiyanto Endri Murni Hati Rukhi Hasibah Tugas: Bahasa Inggris (Narrative Text)Wiyan Alwaysfans CheLseaPas encore d'évaluation
- 3 Growing in FaithDocument5 pages3 Growing in FaithJohnny PadernalPas encore d'évaluation
- Implementation Plan SLRPDocument6 pagesImplementation Plan SLRPAngelina SantosPas encore d'évaluation
- Victron Orion-Tr - Smart - DC-DC - Charger-Manual Non IsolatedDocument19 pagesVictron Orion-Tr - Smart - DC-DC - Charger-Manual Non IsolatedThomist AquinasPas encore d'évaluation
- Principles in Biochemistry (SBK3013)Document3 pagesPrinciples in Biochemistry (SBK3013)Leena MuniandyPas encore d'évaluation
- Vertico SynchroDocument16 pagesVertico SynchrozpramasterPas encore d'évaluation
- Clase No. 24 Nouns and Their Modifiers ExercisesDocument2 pagesClase No. 24 Nouns and Their Modifiers ExercisesenriquefisicoPas encore d'évaluation
- 95491fisa Tehnica Acumulator Growatt Lithiu 6.5 KWH Acumulatori Sistem Fotovoltaic Alaska Energies Romania CompressedDocument4 pages95491fisa Tehnica Acumulator Growatt Lithiu 6.5 KWH Acumulatori Sistem Fotovoltaic Alaska Energies Romania CompressedmiaasieuPas encore d'évaluation
- D435L09 Dental Trauma-2C Cracked Teeth - 26 Root FractureDocument73 pagesD435L09 Dental Trauma-2C Cracked Teeth - 26 Root FractureD YasIr MussaPas encore d'évaluation