Vous aimerez peut-être aussi
- Konsensus HipertiroidDocument6 pagesKonsensus HipertiroidDiethaKusumaningrumPas encore d'évaluation
- Effective Cataract Treatment for AdultsDocument6 pagesEffective Cataract Treatment for AdultsIndra Jati LaksanaPas encore d'évaluation
- Clinical Practice Guideline For CataractDocument27 pagesClinical Practice Guideline For CataractNaufal FarisatriantoPas encore d'évaluation
- Sopt 3Document5 pagesSopt 3Naufal FarisatriantoPas encore d'évaluation
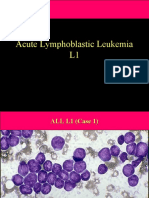
- Acute Lymphoblastic Leukemia L1Document75 pagesAcute Lymphoblastic Leukemia L1Naufal Farisatrianto100% (1)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Cardiopulmonary Resuscitation in Low-Resource SettingsDocument10 pagesCardiopulmonary Resuscitation in Low-Resource SettingsVICTORIA GONZALES ESPADAPas encore d'évaluation
- AfpDocument17 pagesAfpHaris QurashiPas encore d'évaluation
- Efficient Antibiotic Bead Production TechniqueDocument5 pagesEfficient Antibiotic Bead Production Techniqueratnav_ratanPas encore d'évaluation
- Double Crush SyndromeDocument14 pagesDouble Crush SyndromeJosip SulenticPas encore d'évaluation
- Intramedullary Nailing TechniquesDocument94 pagesIntramedullary Nailing TechniquesYasmina Qabbani100% (1)
- Explicative Cases of Controversial Issues in NeurosurgeryDocument544 pagesExplicative Cases of Controversial Issues in NeurosurgeryJosé Ramírez100% (2)
- Presentation RDocument18 pagesPresentation RRaveesh KumarPas encore d'évaluation
- Plan of The Course Anatomy and Clinical Anatomy: Academic Year 2013/2014Document7 pagesPlan of The Course Anatomy and Clinical Anatomy: Academic Year 2013/2014Rinor MujajPas encore d'évaluation
- Evidence Based PracticeDocument11 pagesEvidence Based Practicedana-samer100% (2)
- Administering Intramuscular Injections To Children - What Does The Evidence Say?Document8 pagesAdministering Intramuscular Injections To Children - What Does The Evidence Say?ZACHARIAH MANKIRPas encore d'évaluation
- Presentation On Current Principles and Practices of Pediatric NursingDocument18 pagesPresentation On Current Principles and Practices of Pediatric Nursingmalleshwari athramPas encore d'évaluation
- Dfu For VicmoDocument40 pagesDfu For VicmoAndreea L. MihalceaPas encore d'évaluation
- File 925Document26 pagesFile 925SadishPas encore d'évaluation
- Quiz 2 - Healthcare Quality and Patient SafetyDocument3 pagesQuiz 2 - Healthcare Quality and Patient SafetyRaviraj Pishe100% (1)
- MMDSTDocument2 pagesMMDSTBianca MolinaPas encore d'évaluation
- Thyroid Ultrasound For Thyroidologists: Durr-e-SabihDocument49 pagesThyroid Ultrasound For Thyroidologists: Durr-e-SabihMakmun RadPas encore d'évaluation
- ResumeDocument3 pagesResumeapi-301877122Pas encore d'évaluation
- Apert Syndrome: A Case ReportDocument8 pagesApert Syndrome: A Case ReportIJAR JOURNALPas encore d'évaluation
- Anatomy and Physiology IIDocument13 pagesAnatomy and Physiology IIAuddyjie Hush67% (3)
- NIDCD Noise Induced Hearing LossDocument4 pagesNIDCD Noise Induced Hearing LossquuyiixPas encore d'évaluation
- Bimaxillary Dentoalveolar Protrusion Traits andDocument7 pagesBimaxillary Dentoalveolar Protrusion Traits andSAM PRASANTHPas encore d'évaluation
- SCNICU Starter PackDocument7 pagesSCNICU Starter PackALIF HAIQAL MOHD HUSSEINPas encore d'évaluation
- Care of The High Risk NewbornDocument309 pagesCare of The High Risk NewbornClaire Alvarez OngchuaPas encore d'évaluation
- LCP Técnica PreservaciónDocument6 pagesLCP Técnica PreservacióndrjorgewtorresPas encore d'évaluation
- DH SOP LaQshyaDocument81 pagesDH SOP LaQshyakparasher100% (1)
- 1 s2.0 S0022347616004376 MainDocument7 pages1 s2.0 S0022347616004376 MainRatih KusumawardaniPas encore d'évaluation
- Introduction To LOINC RSNA PlaybookDocument38 pagesIntroduction To LOINC RSNA PlaybookDaniel VreemanPas encore d'évaluation
- Ross ScoreDocument7 pagesRoss Scoreradwika antyPas encore d'évaluation
- Raja Rajeshwari Medical CollegeDocument11 pagesRaja Rajeshwari Medical CollegepentagoneducationPas encore d'évaluation
- Acute Respiratory Distress Syndrome - The Berlin Definition.Document8 pagesAcute Respiratory Distress Syndrome - The Berlin Definition.drschutterPas encore d'évaluation