Vous aimerez peut-être aussi
- Leaping the Hurdles: The Essential Companion Guide for International Medical Graduates on their Australian JourneyD'EverandLeaping the Hurdles: The Essential Companion Guide for International Medical Graduates on their Australian JourneyPas encore d'évaluation
- Case Study 1Document9 pagesCase Study 1andry natanel tonyPas encore d'évaluation
- Mock Osce Midwifery Toc 2021 v2 4 PDFDocument43 pagesMock Osce Midwifery Toc 2021 v2 4 PDFIsse abdikarim ShaiyePas encore d'évaluation
- Intercollegiate Surgical Curriculum ENTDocument98 pagesIntercollegiate Surgical Curriculum ENTMendhi Ashish AnilPas encore d'évaluation
- Scale For The Assessment and Rating of Ataxia (SARA) : 1) Gait 2) StanceDocument2 pagesScale For The Assessment and Rating of Ataxia (SARA) : 1) Gait 2) StancetrcoskiPas encore d'évaluation
- Mock Osce Rn3 Toc 2021 v1.1Document37 pagesMock Osce Rn3 Toc 2021 v1.1Lowri100% (1)
- NMC CBT ExamDocument22 pagesNMC CBT ExamLive PhotosPas encore d'évaluation
- Mock ScenarioDocument35 pagesMock ScenarioCarla Catrina EstradaPas encore d'évaluation
- Written Component Practice Questions enDocument19 pagesWritten Component Practice Questions enNelizaPas encore d'évaluation
- Introduction To Nursing Research Part 1Document22 pagesIntroduction To Nursing Research Part 1Ciedelle Honey Lou DimaligPas encore d'évaluation
- Student Satisfaction Questionnaire (1) .Doc 03Document2 pagesStudent Satisfaction Questionnaire (1) .Doc 03Puspa NathanPas encore d'évaluation
- (Osborn) Chapter 73 Learning Outcomes (Number and Title)Document16 pages(Osborn) Chapter 73 Learning Outcomes (Number and Title)KittiesPas encore d'évaluation
- Scope of Practice For RN DHA PDFDocument18 pagesScope of Practice For RN DHA PDFRrichard Prieto MmallariPas encore d'évaluation
- 441 N Pos Ce Candidate GuidebookDocument23 pages441 N Pos Ce Candidate GuidebookVeronica ErlinPas encore d'évaluation
- Standards of Proficiency PhysiotherapistsDocument20 pagesStandards of Proficiency PhysiotherapistsFaisal QureshiPas encore d'évaluation
- Pharmacodynamics and Pharmacokinetics Quiz 14 - 20Document12 pagesPharmacodynamics and Pharmacokinetics Quiz 14 - 20Killer VPas encore d'évaluation
- Guide For Overseas Applicants IRELAND PDFDocument29 pagesGuide For Overseas Applicants IRELAND PDFJasonLeePas encore d'évaluation
- Mock Osce Rn1 Toc 2021 v1.1Document42 pagesMock Osce Rn1 Toc 2021 v1.1Ameng GosimPas encore d'évaluation
- Course OutlineNUR 1113 - Professional Nursing 2011-12 Sem 1studentDocument4 pagesCourse OutlineNUR 1113 - Professional Nursing 2011-12 Sem 1studentNurul AiniPas encore d'évaluation
- The New Doctor 09Document52 pagesThe New Doctor 09Almas JanjuaPas encore d'évaluation
- Communication Skills For Final MB A Guide To Success in The Osce PDFDocument2 pagesCommunication Skills For Final MB A Guide To Success in The Osce PDFRahulPas encore d'évaluation
- APTA Professionalism Core Values Self AssessmentDocument11 pagesAPTA Professionalism Core Values Self AssessmentJPPas encore d'évaluation
- NRSG 7010 SyllabusDocument6 pagesNRSG 7010 Syllabusapi-310557802Pas encore d'évaluation
- Blood Gas Book Workbook 2008Document41 pagesBlood Gas Book Workbook 2008May Boonpeng100% (1)
- Preparing-For-Your-Osce - All-Nursing-Fields-2021 M TawaklDocument17 pagesPreparing-For-Your-Osce - All-Nursing-Fields-2021 M Tawaklloave.mando.7Pas encore d'évaluation
- 34 Ms Surgery LogbookDocument111 pages34 Ms Surgery LogbookMohamedHossam50% (2)
- ReflectionDocument3 pagesReflectionapi-238773232Pas encore d'évaluation
- F2 Stand-Alone SJT Practice ScenariosDocument4 pagesF2 Stand-Alone SJT Practice ScenariosKing GodwinPas encore d'évaluation
- OET - Parts of The ExamDocument5 pagesOET - Parts of The ExamLiz ColoPas encore d'évaluation
- Improvement in Documentation of Intake and Output ChartDocument2 pagesImprovement in Documentation of Intake and Output ChartanurajonePas encore d'évaluation
- Sample Questions Asked in Interview KCRDocument2 pagesSample Questions Asked in Interview KCRPopa NiculinaPas encore d'évaluation
- Adaptation Nurse Job DescriptionDocument12 pagesAdaptation Nurse Job DescriptionM LubisPas encore d'évaluation
- 84 Questions - With Answer - Gloucestershire HospitalsDocument171 pages84 Questions - With Answer - Gloucestershire HospitalsŞahin EmerPas encore d'évaluation
- Strategies of TeachingDocument34 pagesStrategies of TeachingallanPas encore d'évaluation
- Fon 1Document26 pagesFon 1fulltimepapi100% (1)
- 205 Principles of SafeguardingDocument16 pages205 Principles of SafeguardingUnCalatorPas encore d'évaluation
- Organizational Behaviour: Bba & BHMDocument249 pagesOrganizational Behaviour: Bba & BHMKhushi NaharPas encore d'évaluation
- Evaluating The Neurologic Status of Unconscious PatientDocument3 pagesEvaluating The Neurologic Status of Unconscious Patientsambel_88Pas encore d'évaluation
- NCM 113 CHN 2-Midterms-ReviewerDocument9 pagesNCM 113 CHN 2-Midterms-ReviewerKIRSTEN CHAVEZPas encore d'évaluation
- Standards For Nursing EducationDocument7 pagesStandards For Nursing Educationemir_bautista2002Pas encore d'évaluation
- Early Clinical Exposure (Ece)Document30 pagesEarly Clinical Exposure (Ece)sandeepPas encore d'évaluation
- Rcsed Mrcs Guide v6Document12 pagesRcsed Mrcs Guide v6Min MawPas encore d'évaluation
- Zimmer Biomet ANZ Fellowship Directory 2019Document22 pagesZimmer Biomet ANZ Fellowship Directory 2019FahadPas encore d'évaluation
- HAAD-Policy Scope of Practice For Practical Nurse PDFDocument4 pagesHAAD-Policy Scope of Practice For Practical Nurse PDFmyangel_peach3305Pas encore d'évaluation
- Nurs 603 Assignment 1 Objective Tests Design and Considerations Final For SubmissionDocument13 pagesNurs 603 Assignment 1 Objective Tests Design and Considerations Final For Submissionapi-323169345Pas encore d'évaluation
- Example of An Osce Ospe Examination BookDocument51 pagesExample of An Osce Ospe Examination BookLouise Tan100% (3)
- B. Sent It To ArchiveDocument74 pagesB. Sent It To Archiveoluyemi7iwalola7ifejPas encore d'évaluation
- Interview Questions To PrepareDocument7 pagesInterview Questions To Prepareico_isPas encore d'évaluation
- BSN Learning Plan Senior CapstoneDocument3 pagesBSN Learning Plan Senior Capstoneapi-258684779100% (1)
- Doctor Patient RealationshipDocument9 pagesDoctor Patient RealationshipSara EamranPas encore d'évaluation
- CBT 2020 PremDocument33 pagesCBT 2020 Premபிரேம் குமார் ராஜாமணிPas encore d'évaluation
- Factors Related To Health PromotionDocument25 pagesFactors Related To Health PromotionKillian SibzPas encore d'évaluation
- CSP Core Standards 2005 0Document68 pagesCSP Core Standards 2005 0Irina MafteiPas encore d'évaluation
- MSRA SJT Glossary Terms 2022-23 FINAL 2023Document10 pagesMSRA SJT Glossary Terms 2022-23 FINAL 2023blatantly fakePas encore d'évaluation
- Early AdulthoodDocument1 pageEarly AdulthoodCherry BobierPas encore d'évaluation
- Job DescriptionDocument10 pagesJob Descriptionpioneer92Pas encore d'évaluation
- Class 1 Introduction To Clinical PharmacologyDocument33 pagesClass 1 Introduction To Clinical Pharmacologymustafa 1Pas encore d'évaluation
- Faculty DevlopmentDocument3 pagesFaculty Devlopmentapi-257865334Pas encore d'évaluation
- Exam Administration and AnalysisDocument5 pagesExam Administration and Analysisapi-257865334Pas encore d'évaluation
- ClinicalevalfinalDocument3 pagesClinicalevalfinalapi-257865334Pas encore d'évaluation
- Stacygallegos The KWL Chart 2Document2 pagesStacygallegos The KWL Chart 2api-257865334Pas encore d'évaluation
- Buy Augmentin 1000 - AllDayGenericDocument7 pagesBuy Augmentin 1000 - AllDayGenericBonitaPas encore d'évaluation
- Cervical DystociaDocument22 pagesCervical DystociaBaldau TiwariPas encore d'évaluation
- Pandemic vs. NeurodivergenceDocument5 pagesPandemic vs. NeurodivergenceEuan PasamontePas encore d'évaluation
- CHN DOH ProgramsDocument158 pagesCHN DOH Programsjudd wilson100% (1)
- Urinary System RadiographyDocument32 pagesUrinary System RadiographyVivek ChaudharyPas encore d'évaluation
- Case PresentationDocument11 pagesCase PresentationHira Rafique100% (1)
- Gynecology Adnexal MassDocument2 pagesGynecology Adnexal MassgePas encore d'évaluation
- Dmso Natures Best HealerDocument2 pagesDmso Natures Best HealerJan Pran100% (1)
- TESDA COVID-19 Test (Answer Keys)Document12 pagesTESDA COVID-19 Test (Answer Keys)ash mizushiPas encore d'évaluation
- Thesis Statement Examples For Eating DisordersDocument6 pagesThesis Statement Examples For Eating Disordersjenniferontiveroskansascity100% (2)
- Microbiology Question PapersDocument100 pagesMicrobiology Question Papersprinceej92% (13)
- UCDocument6 pagesUCapiv2010_808955526Pas encore d'évaluation
- Paracetamol - DSDocument3 pagesParacetamol - DSEnoch LabianoPas encore d'évaluation
- Test Bank For Clinical Laboratory Hematology 2nd Edition MckenzieDocument12 pagesTest Bank For Clinical Laboratory Hematology 2nd Edition Mckenzienoumenalskall0wewPas encore d'évaluation
- Connors and Other ADHD ScalesDocument3 pagesConnors and Other ADHD ScalesPragnya NidugondaPas encore d'évaluation
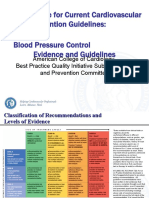
- 3 ACC Prevention Blood PressureDocument69 pages3 ACC Prevention Blood PressureMelissa Delgado100% (1)
- Gonzaga Rlems - NCPDocument3 pagesGonzaga Rlems - NCPShaynne Wencille A. GONZAGAPas encore d'évaluation
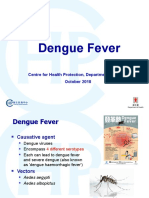
- Dengue Fever (Nepal) An Emerging Public Health Problem.Document13 pagesDengue Fever (Nepal) An Emerging Public Health Problem.Bzay DhitalPas encore d'évaluation
- Dengue Fever EngDocument17 pagesDengue Fever EngRia Tustina HendrayaniPas encore d'évaluation
- Artikel Bahan Ujian PraktikumDocument10 pagesArtikel Bahan Ujian PraktikumTakiaGenjiPas encore d'évaluation
- Rectal ProlapseDocument2 pagesRectal ProlapseSalem ZoghbyPas encore d'évaluation
- 04 GTTDocument15 pages04 GTTAshish TuralePas encore d'évaluation
- Fatigue After StrokeDocument6 pagesFatigue After StrokeAnugerah NasutionPas encore d'évaluation
- Global Urology Devices MarketDocument14 pagesGlobal Urology Devices MarketNamrataPas encore d'évaluation
- LUMOS - DementiaDocument100 pagesLUMOS - DementiasamuelPas encore d'évaluation
- Liver BiopsyDocument4 pagesLiver BiopsyLouis FortunatoPas encore d'évaluation
- Cardiac Enzymes - KulDocument39 pagesCardiac Enzymes - KulAnonymous J1iWk2xPas encore d'évaluation
- s12944 022 01717 8Document15 pagess12944 022 01717 8IZAMAR NADDINE LLAURE FLORESPas encore d'évaluation
- Daftar Pustaka Semua 1-4Document8 pagesDaftar Pustaka Semua 1-4Yuni IsnayantiPas encore d'évaluation
- Family Medicine Clerkship Logbook G3 FinalDocument76 pagesFamily Medicine Clerkship Logbook G3 FinalMohammed AlomarPas encore d'évaluation
- Stoicism The Art of Happiness: How the Stoic Philosophy Works, Living a Good Life, Finding Calm and Managing Your Emotions in a Turbulent World. New VersionD'EverandStoicism The Art of Happiness: How the Stoic Philosophy Works, Living a Good Life, Finding Calm and Managing Your Emotions in a Turbulent World. New VersionÉvaluation : 5 sur 5 étoiles5/5 (51)
- Weapons of Mass Instruction: A Schoolteacher's Journey Through the Dark World of Compulsory SchoolingD'EverandWeapons of Mass Instruction: A Schoolteacher's Journey Through the Dark World of Compulsory SchoolingÉvaluation : 4.5 sur 5 étoiles4.5/5 (149)
- Summary: The Laws of Human Nature: by Robert Greene: Key Takeaways, Summary & AnalysisD'EverandSummary: The Laws of Human Nature: by Robert Greene: Key Takeaways, Summary & AnalysisÉvaluation : 4.5 sur 5 étoiles4.5/5 (30)
- Follow your interests: This will make you feel better about yourself and what you can do.: inspiration and wisdom for achieving a fulfilling life.D'EverandFollow your interests: This will make you feel better about yourself and what you can do.: inspiration and wisdom for achieving a fulfilling life.Pas encore d'évaluation
- How to Improve English Speaking: How to Become a Confident and Fluent English SpeakerD'EverandHow to Improve English Speaking: How to Become a Confident and Fluent English SpeakerÉvaluation : 4.5 sur 5 étoiles4.5/5 (56)
- Summary: Trading in the Zone: Trading in the Zone: Master the Market with Confidence, Discipline, and a Winning Attitude by Mark Douglas: Key Takeaways, Summary & AnalysisD'EverandSummary: Trading in the Zone: Trading in the Zone: Master the Market with Confidence, Discipline, and a Winning Attitude by Mark Douglas: Key Takeaways, Summary & AnalysisÉvaluation : 5 sur 5 étoiles5/5 (15)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipD'EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipÉvaluation : 4.5 sur 5 étoiles4.5/5 (1135)
- Learn Spanish While SleepingD'EverandLearn Spanish While SleepingÉvaluation : 4 sur 5 étoiles4/5 (20)
- Summary: The 5AM Club: Own Your Morning. Elevate Your Life. by Robin Sharma: Key Takeaways, Summary & AnalysisD'EverandSummary: The 5AM Club: Own Your Morning. Elevate Your Life. by Robin Sharma: Key Takeaways, Summary & AnalysisÉvaluation : 4.5 sur 5 étoiles4.5/5 (22)
- Summary: I'm Glad My Mom Died: by Jennette McCurdy: Key Takeaways, Summary & AnalysisD'EverandSummary: I'm Glad My Mom Died: by Jennette McCurdy: Key Takeaways, Summary & AnalysisÉvaluation : 4.5 sur 5 étoiles4.5/5 (2)
- Dumbing Us Down: The Hidden Curriculum of Compulsory SchoolingD'EverandDumbing Us Down: The Hidden Curriculum of Compulsory SchoolingÉvaluation : 4.5 sur 5 étoiles4.5/5 (498)
- The Story of the World, Vol. 1 AudiobookD'EverandThe Story of the World, Vol. 1 AudiobookÉvaluation : 4.5 sur 5 étoiles4.5/5 (3)
- The 16 Undeniable Laws of Communication: Apply Them and Make the Most of Your MessageD'EverandThe 16 Undeniable Laws of Communication: Apply Them and Make the Most of Your MessageÉvaluation : 5 sur 5 étoiles5/5 (73)
- Make It Stick by Peter C. Brown, Henry L. Roediger III, Mark A. McDaniel - Book Summary: The Science of Successful LearningD'EverandMake It Stick by Peter C. Brown, Henry L. Roediger III, Mark A. McDaniel - Book Summary: The Science of Successful LearningÉvaluation : 4.5 sur 5 étoiles4.5/5 (55)
- The Story of the World, Vol. 2 AudiobookD'EverandThe Story of the World, Vol. 2 AudiobookÉvaluation : 5 sur 5 étoiles5/5 (2)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisD'EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisÉvaluation : 5 sur 5 étoiles5/5 (3)
- Summary: Dotcom Secrets: The Underground Playbook for Growing Your Company Online with Sales Funnels by Russell Brunson: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: Dotcom Secrets: The Underground Playbook for Growing Your Company Online with Sales Funnels by Russell Brunson: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (2)
- Cynical Theories: How Activist Scholarship Made Everything about Race, Gender, and Identity―and Why This Harms EverybodyD'EverandCynical Theories: How Activist Scholarship Made Everything about Race, Gender, and Identity―and Why This Harms EverybodyÉvaluation : 4.5 sur 5 étoiles4.5/5 (221)
- Summary: Greenlights: by Matthew McConaughey: Key Takeaways, Summary & AnalysisD'EverandSummary: Greenlights: by Matthew McConaughey: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (6)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4.5 sur 5 étoiles4.5/5 (1875)
- Learn Japanese - Level 1: Introduction to Japanese, Volume 1: Volume 1: Lessons 1-25D'EverandLearn Japanese - Level 1: Introduction to Japanese, Volume 1: Volume 1: Lessons 1-25Évaluation : 5 sur 5 étoiles5/5 (17)
- Rooted in Joy: Creating a Classroom Culture of Equity, Belonging, and CareD'EverandRooted in Joy: Creating a Classroom Culture of Equity, Belonging, and CarePas encore d'évaluation
- You Are Not Special: And Other EncouragementsD'EverandYou Are Not Special: And Other EncouragementsÉvaluation : 4.5 sur 5 étoiles4.5/5 (6)
- Financial Feminist: Overcome the Patriarchy's Bullsh*t to Master Your Money and Build a Life You LoveD'EverandFinancial Feminist: Overcome the Patriarchy's Bullsh*t to Master Your Money and Build a Life You LoveÉvaluation : 5 sur 5 étoiles5/5 (1)
- Little Soldiers: An American Boy, a Chinese School, and the Global Race to AchieveD'EverandLittle Soldiers: An American Boy, a Chinese School, and the Global Race to AchieveÉvaluation : 4 sur 5 étoiles4/5 (25)