Vous aimerez peut-être aussi
- AFS Casting Defect HandbookDocument119 pagesAFS Casting Defect Handbooktyagimanoj90100% (7)
- Intervention Radiology ProceduresDocument58 pagesIntervention Radiology Proceduresjusttesting10Pas encore d'évaluation
- Acr Mri BiradsDocument3 pagesAcr Mri BiradsFilipe BarraPas encore d'évaluation
- Chapter 1 - Differential EquationsDocument27 pagesChapter 1 - Differential EquationsAbdul AddaharyPas encore d'évaluation
- Introduction To Imaging and Radiologic ScienceDocument18 pagesIntroduction To Imaging and Radiologic ScienceminayokiPas encore d'évaluation
- Women's Imaging: MRI with Multimodality CorrelationD'EverandWomen's Imaging: MRI with Multimodality CorrelationMichele A. BrownÉvaluation : 5 sur 5 étoiles5/5 (1)
- Slips PreventionDocument12 pagesSlips Preventionapi-270822363Pas encore d'évaluation
- Project Report CharlotteHaumanDocument79 pagesProject Report CharlotteHaumanRodger OlynPas encore d'évaluation
- Radiology Physics Board Recalls 2005Document14 pagesRadiology Physics Board Recalls 2005Turki A. Saad100% (2)
- Aerodyn Aeronaut and Fligh MechDocument664 pagesAerodyn Aeronaut and Fligh MechAerospaceAngel100% (5)
- Behrens - Physical Agents Theory and Practice, 3E PDFDocument473 pagesBehrens - Physical Agents Theory and Practice, 3E PDFtin67% (3)
- Chapter 3 Work and Energy MethodDocument23 pagesChapter 3 Work and Energy Methoddudescape100% (1)
- Module - I: JurisprudenceDocument10 pagesModule - I: JurisprudenceReygil CapunoPas encore d'évaluation
- Iodinated Contrast Media GuidelineDocument41 pagesIodinated Contrast Media GuidelineN Aa100% (1)
- Atlas of Hybrid Imaging Sectional Anatomy for PET/CT, PET/MRI and SPECT/CT Vol. 2: Thorax Abdomen and Pelvis: Sectional Anatomy for PET/CT, PET/MRI and SPECT/CTD'EverandAtlas of Hybrid Imaging Sectional Anatomy for PET/CT, PET/MRI and SPECT/CT Vol. 2: Thorax Abdomen and Pelvis: Sectional Anatomy for PET/CT, PET/MRI and SPECT/CTPas encore d'évaluation
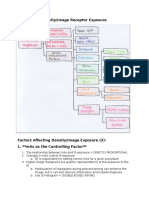
- Chapter 26: Density/Image Receptor Exposure: Notebook #7Document8 pagesChapter 26: Density/Image Receptor Exposure: Notebook #7api-338781568Pas encore d'évaluation
- TestBank c1Document7 pagesTestBank c1rehab ebraheemPas encore d'évaluation
- VMARTDocument92 pagesVMARTCyc XimenaPas encore d'évaluation
- Resident Physics Lectures: Radiography GeometryDocument36 pagesResident Physics Lectures: Radiography GeometryLajja Parikh PatelPas encore d'évaluation
- Radiology ReviewerDocument26 pagesRadiology ReviewerSean Jodi CosepePas encore d'évaluation
- Hydrogen Permeability and Integrity of Hydrogen Transfer PipelinesDocument52 pagesHydrogen Permeability and Integrity of Hydrogen Transfer PipelineslaercioudescPas encore d'évaluation
- Breast 2014Document9 pagesBreast 2014SyedPas encore d'évaluation
- Contrast MediaDocument94 pagesContrast MediaJustin JosePas encore d'évaluation
- Conventional RadiologyDocument2 pagesConventional RadiologyPier Cedron LescanoPas encore d'évaluation
- Grids and Scatter ReductionDocument79 pagesGrids and Scatter ReductionMondiaal Financial ServicesPas encore d'évaluation
- Samples of Test Bank For Introduction To Radiologic and Imaging Sciences and Patient Care 6th Edition by Arlene M. AdlerDocument4 pagesSamples of Test Bank For Introduction To Radiologic and Imaging Sciences and Patient Care 6th Edition by Arlene M. AdlerRHEA T MACANILAOPas encore d'évaluation
- Medical AuditDocument9 pagesMedical AuditKailash NagarPas encore d'évaluation
- Liver Imaging: MRI with CT CorrelationD'EverandLiver Imaging: MRI with CT CorrelationErsan AltunPas encore d'évaluation
- BI-RADS For UltrasonographyDocument11 pagesBI-RADS For UltrasonographyLucas GuadaPas encore d'évaluation
- Manoeuvring The Vessels in Heavy Weather at SeaDocument7 pagesManoeuvring The Vessels in Heavy Weather at SeaMahesh Poonia100% (5)
- 103manual QAP Radiologi Pindaan Januari 2019Document115 pages103manual QAP Radiologi Pindaan Januari 2019UMGC Sri RampaiPas encore d'évaluation
- Lab Report Pump PerformanceDocument20 pagesLab Report Pump Performanceamirshafiq67% (3)
- Carriculum MainDocument159 pagesCarriculum Maingaashe100% (1)
- Anatomy Imaging For Radiotherapy PDFDocument41 pagesAnatomy Imaging For Radiotherapy PDFIkang FauziPas encore d'évaluation
- OHS Body of Knowledge Risk April, 2012Document50 pagesOHS Body of Knowledge Risk April, 2012amirq4Pas encore d'évaluation
- Radiology Lectures on Udemy for Medical Imaging ExamsDocument1 pageRadiology Lectures on Udemy for Medical Imaging ExamsSrirupa BiswasPas encore d'évaluation
- Contrast Media Administration Guidelines by The ACR (American College of Radiology) Version 6 - 2008Document92 pagesContrast Media Administration Guidelines by The ACR (American College of Radiology) Version 6 - 2008radiology_resources100% (25)
- Essential Guidelines for Trauma RadiographyDocument69 pagesEssential Guidelines for Trauma RadiographySyuhada AzmiPas encore d'évaluation
- Physicspreview PDFDocument44 pagesPhysicspreview PDFEstrella Peuvé100% (1)
- 2012 ASTRO Radiation and Cancer Biology Practice Examination and Study Guide PDFDocument193 pages2012 ASTRO Radiation and Cancer Biology Practice Examination and Study Guide PDFKoustav Majumder100% (2)
- Maintenance Engineer PDFDocument4 pagesMaintenance Engineer PDFMasroor RasoolPas encore d'évaluation
- Basarab Nicolescu, The Relationship Between Complex Thinking and TransdisciplinarityDocument17 pagesBasarab Nicolescu, The Relationship Between Complex Thinking and TransdisciplinarityBasarab Nicolescu100% (2)
- Physical Principles of UtzDocument44 pagesPhysical Principles of UtzRalph RichardPas encore d'évaluation
- Assessing The Status of Professional Ethics Among Ghanaian RadiographersDocument31 pagesAssessing The Status of Professional Ethics Among Ghanaian Radiographersdeehans100% (1)
- Interpretation of Magnetic Resonance Imaging of Orbit: Simplifi Ed For Ophthalmologists (Part I)Document7 pagesInterpretation of Magnetic Resonance Imaging of Orbit: Simplifi Ed For Ophthalmologists (Part I)Abid AliPas encore d'évaluation
- CAMRT Book ListDocument2 pagesCAMRT Book Listমেডিকেল বুকস্ হাউজ33% (3)
- Week 9 C Chapter 40 Radiation Protection, Chapter 31 QC 84Document84 pagesWeek 9 C Chapter 40 Radiation Protection, Chapter 31 QC 84chicken66Pas encore d'évaluation
- CME1020 RadiologyDocument10 pagesCME1020 Radiologyeternal sunshinePas encore d'évaluation
- Accutron HPDocument6 pagesAccutron HPsensaadPas encore d'évaluation
- Radiology Request Forms ResearchDocument8 pagesRadiology Request Forms Researchtruevine_ministryPas encore d'évaluation
- European Guidelines On Quality Criteria For Computed Tomography PDFDocument2 pagesEuropean Guidelines On Quality Criteria For Computed Tomography PDFBennettPas encore d'évaluation
- MD RadiodiagnosisDocument12 pagesMD RadiodiagnosisPravin TamminanaPas encore d'évaluation
- Evaluation of Plan Dosimetry Using Scoring Index For Prostate Intensity-Modulated Radiation Therapy (Imrt)Document1 pageEvaluation of Plan Dosimetry Using Scoring Index For Prostate Intensity-Modulated Radiation Therapy (Imrt)Saad SaeedPas encore d'évaluation
- Biological Effects of UltrasoundDocument3 pagesBiological Effects of UltrasoundSaravjeet Singh100% (1)
- Principles of Exposure Ch.8Document42 pagesPrinciples of Exposure Ch.8abdulsalam khalaf100% (1)
- Clinical Training MP Specializing in Radiation OncologyDocument225 pagesClinical Training MP Specializing in Radiation Oncologyjiar001Pas encore d'évaluation
- Basic RadiologyDocument27 pagesBasic RadiologyYuanna Liilio PedrosaPas encore d'évaluation
- Job Responsibility Checklist - RadiogrpherDocument2 pagesJob Responsibility Checklist - Radiogrphertafi66Pas encore d'évaluation
- FC Rad Diag (SA) Part I Past Papers - 2019 2nd Semester 3 1 2020Document2 pagesFC Rad Diag (SA) Part I Past Papers - 2019 2nd Semester 3 1 2020Mo CajeePas encore d'évaluation
- Viner 2005 Forensic Radiography in South AfricaDocument24 pagesViner 2005 Forensic Radiography in South Africah8517Pas encore d'évaluation
- Radiation Protection For PatientDocument2 pagesRadiation Protection For PatientLenaCPas encore d'évaluation
- 05 Birads Us Reporting Acr 2013Document12 pages05 Birads Us Reporting Acr 2013shilacorinaPas encore d'évaluation
- Master's in Radiodiagnosis Program GuideDocument149 pagesMaster's in Radiodiagnosis Program GuideAhmeid Eid0% (1)
- 2 Fundamental Principles of RadiobiologyDocument28 pages2 Fundamental Principles of RadiobiologyAngelo RamosPas encore d'évaluation
- Physics of Radiation - Lec1Document10 pagesPhysics of Radiation - Lec1شبكة المستقبلPas encore d'évaluation
- Rtog 0813 Marina CousinsDocument22 pagesRtog 0813 Marina Cousinsapi-426094285Pas encore d'évaluation
- UZVDocument56 pagesUZVGoran MaliPas encore d'évaluation
- Quality Assurance in Radiation DosimetryDocument9 pagesQuality Assurance in Radiation DosimetrydinkarvermaPas encore d'évaluation
- TCS-47 Web PDFDocument246 pagesTCS-47 Web PDFMady BuzeaPas encore d'évaluation
- (Philip T. English DCR, Christine Moore DCR (Auth.Document188 pages(Philip T. English DCR, Christine Moore DCR (Auth.Åri Budianto100% (1)
- ProposalDocument22 pagesProposalKD CarlosPas encore d'évaluation
- Prevention of Noise InducedDocument14 pagesPrevention of Noise Inducedapi-270822363Pas encore d'évaluation
- Radiation Control Measures 2Document25 pagesRadiation Control Measures 2api-270822363Pas encore d'évaluation
- Noise Control ArticleDocument8 pagesNoise Control Articleapi-270822363Pas encore d'évaluation
- Radiation StandardDocument28 pagesRadiation Standardapi-270822363Pas encore d'évaluation
- Radiation Exposure Standard1Document83 pagesRadiation Exposure Standard1api-270822363Pas encore d'évaluation
- Radiation Control in SpaceDocument7 pagesRadiation Control in Spaceapi-270822363Pas encore d'évaluation
- Science Os Slips Falls and TripsDocument8 pagesScience Os Slips Falls and Tripsapi-270822363Pas encore d'évaluation
- Preventing Slips NSWDocument24 pagesPreventing Slips NSWapi-270822363Pas encore d'évaluation
- Managing The Risk of Falls at WorkplacesDocument54 pagesManaging The Risk of Falls at Workplacesceliofsilva8993Pas encore d'évaluation
- Radiation Protection and ControlDocument169 pagesRadiation Protection and Controlapi-270822363Pas encore d'évaluation
- Trips PreventionDocument2 pagesTrips Preventionapi-270822363Pas encore d'évaluation
- Guide For Preventing Slips ComcareDocument24 pagesGuide For Preventing Slips Comcareapi-270822363Pas encore d'évaluation
- Slips and Falls HazardsDocument6 pagesSlips and Falls Hazardsapi-270822363Pas encore d'évaluation
- Preventing Slips and Falls Through LeisureDocument6 pagesPreventing Slips and Falls Through Leisureapi-270822363Pas encore d'évaluation
- Vibration Induced Whit FeetDocument11 pagesVibration Induced Whit Feetapi-270822363Pas encore d'évaluation
- Preventing Falls UkDocument6 pagesPreventing Falls Ukapi-270822363Pas encore d'évaluation
- Department of Health and AgeingDocument24 pagesDepartment of Health and Ageingapi-270822363Pas encore d'évaluation
- Vhand Arm Vibration FactsheetDocument3 pagesVhand Arm Vibration Factsheetapi-270822363Pas encore d'évaluation
- Vibration Exposure LimitsDocument5 pagesVibration Exposure Limitsapi-270822363Pas encore d'évaluation
- Vibration CalculatorDocument1 pageVibration Calculatorapi-270822363Pas encore d'évaluation
- Hand Arm Vibration SyndromDocument10 pagesHand Arm Vibration Syndromapi-270822363Pas encore d'évaluation
- NHEWS Vibration Exposure Provision Vibration Controls Australian Workplaces July 2010Document67 pagesNHEWS Vibration Exposure Provision Vibration Controls Australian Workplaces July 2010KBPas encore d'évaluation
- Raynauds Men and WomenDocument7 pagesRaynauds Men and Womenapi-270822363Pas encore d'évaluation
- Diagnosis of Raynauds PhenomenonDocument7 pagesDiagnosis of Raynauds Phenomenonapi-270822363Pas encore d'évaluation
- Vibration CalculatorDocument1 pageVibration Calculatorapi-270822363Pas encore d'évaluation
- Noise MeasurementDocument11 pagesNoise Measurementapi-270822363Pas encore d'évaluation
- NHEWS Vibration Exposure Provision Vibration Controls Australian Workplaces July 2010Document67 pagesNHEWS Vibration Exposure Provision Vibration Controls Australian Workplaces July 2010KBPas encore d'évaluation
- TLC Analysis of Siling Labuyo Extract ComponentsDocument3 pagesTLC Analysis of Siling Labuyo Extract ComponentsJan Eric Balete0% (1)
- Optical CommunicationDocument5 pagesOptical CommunicationSaiviswanth BoggarapuPas encore d'évaluation
- 525d Manual Instalare Detector Paradox Cu MicroundeDocument2 pages525d Manual Instalare Detector Paradox Cu MicroundeGheorghiescu AndreiPas encore d'évaluation
- Physics7c Fa00 mt1 Packard ExamDocument2 pagesPhysics7c Fa00 mt1 Packard ExamfrankongPas encore d'évaluation
- Parasitic DragDocument4 pagesParasitic DragsarfraazPas encore d'évaluation
- CmpE Degree RequirementsDocument3 pagesCmpE Degree RequirementsTrai TranPas encore d'évaluation
- Mahesh CP 506Document25 pagesMahesh CP 506GURUDEEP PPas encore d'évaluation
- SupportVectorMachine NotesDocument131 pagesSupportVectorMachine Notesjangli hathiPas encore d'évaluation
- F'edtu: Standard Specification FOR Ceramic Fibre BlanketsDocument6 pagesF'edtu: Standard Specification FOR Ceramic Fibre BlanketsAnonymous dmMjTmyIPas encore d'évaluation
- Leaflet LouvreDocument32 pagesLeaflet LouvreIndra Kurniawan100% (1)
- Semikron Datasheet Skm100gb12t4 22892020Document5 pagesSemikron Datasheet Skm100gb12t4 22892020Mynk Maddy VsvkrmaPas encore d'évaluation
- Form 5A: Term Distribution of Course: ST STDocument3 pagesForm 5A: Term Distribution of Course: ST STFrances TangubPas encore d'évaluation
- Solid Solution HardeningDocument5 pagesSolid Solution HardeningVasantha SudasinghaPas encore d'évaluation
- Answers To Specific Heat ProblemsDocument5 pagesAnswers To Specific Heat ProblemsSiraj AL sharifPas encore d'évaluation
- Mechanical Engineering Third Semester Exam SolutionsDocument4 pagesMechanical Engineering Third Semester Exam SolutionsJASON CHERIAN MEPas encore d'évaluation
- Laboratory Manual Course Code Ece254 Course Title: Unified Electronics Laboratory-IDocument67 pagesLaboratory Manual Course Code Ece254 Course Title: Unified Electronics Laboratory-IKaran SainiPas encore d'évaluation
- Journal of Petroleum Science and EngineeringDocument13 pagesJournal of Petroleum Science and EngineeringEzequiel AbrilPas encore d'évaluation
- 5 Longitudinal and Transverse VibrationsDocument4 pages5 Longitudinal and Transverse Vibrationsenggsantu0% (1)
- IJIRAE::An Overviewof Analysis, Measurement and Modelling of Dynamics Properties of Composite Materials Using Oberst Beam MethodDocument4 pagesIJIRAE::An Overviewof Analysis, Measurement and Modelling of Dynamics Properties of Composite Materials Using Oberst Beam MethodIJIRAE- International Journal of Innovative Research in Advanced EngineeringPas encore d'évaluation
- Computer SylDocument87 pagesComputer Sylambuj2011Pas encore d'évaluation