Vous aimerez peut-être aussi
- Prostate Imrt Vs VmatDocument20 pagesProstate Imrt Vs Vmatapi-281921437Pas encore d'évaluation
- Alyssa Mellott ResumeDocument2 pagesAlyssa Mellott Resumeapi-281921437Pas encore d'évaluation
- The Ohio State University Radiation Therapy CT Simulation Competency Evaluations Class of 2012-2014Document1 pageThe Ohio State University Radiation Therapy CT Simulation Competency Evaluations Class of 2012-2014api-278240998Pas encore d'évaluation
- TX CompsDocument3 pagesTX Compsapi-312374730Pas encore d'évaluation
- Head & Neck Case Study: Parotid Gland: Alyssa MellottDocument28 pagesHead & Neck Case Study: Parotid Gland: Alyssa Mellottapi-281921437Pas encore d'évaluation
- Compare-Contrast PaperDocument4 pagesCompare-Contrast Paperapi-281921437Pas encore d'évaluation
- Soft Tissue SarcomaDocument38 pagesSoft Tissue Sarcomaapi-281921437Pas encore d'évaluation
- Acute Lymphoblastic Leukemia: Alyssa MellottDocument26 pagesAcute Lymphoblastic Leukemia: Alyssa Mellottapi-281921437Pas encore d'évaluation
- Annotated BibDocument7 pagesAnnotated Bibapi-281921437Pas encore d'évaluation
- Required 20 Patient 20 Care 20 CompetenciesDocument2 pagesRequired 20 Patient 20 Care 20 Competenciesapi-250260293Pas encore d'évaluation
- Case StudyDocument9 pagesCase Studyapi-281921437Pas encore d'évaluation
- Radiation Safety Following Prostate BrachytherapyDocument7 pagesRadiation Safety Following Prostate Brachytherapyapi-281921437Pas encore d'évaluation
- Veni CompDocument1 pageVeni Compapi-313356122Pas encore d'évaluation
- Required Dosimetry CompetenciesDocument2 pagesRequired Dosimetry Competenciesapi-345373364Pas encore d'évaluation
- Program Outcomes 2014Document3 pagesProgram Outcomes 2014api-278240998Pas encore d'évaluation
- Radtx 15 16 3rd Version-2Document2 pagesRadtx 15 16 3rd Version-2api-281921437Pas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Metodo SOAP para Evoluçao FarmaceuticaDocument6 pagesMetodo SOAP para Evoluçao FarmaceuticaLuis Filipe FerreiraPas encore d'évaluation
- 10 Rights of Drug Administration With Nursing ImplicationsDocument3 pages10 Rights of Drug Administration With Nursing ImplicationsJet Bautista100% (6)
- Drug Study - HydrocortisoneDocument4 pagesDrug Study - Hydrocortisoneryan88% (8)
- Farmacologia Del TramalDocument45 pagesFarmacologia Del TramalJenni Paola CarvajalinoPas encore d'évaluation
- National Drug Policy of Bangladesh 2005Document3 pagesNational Drug Policy of Bangladesh 2005নোমানআবদিল্লাহPas encore d'évaluation
- Directorate General of Drug Administration: SL Name of The Pharmaceutical Address Location Licence No. Present StatusDocument2 pagesDirectorate General of Drug Administration: SL Name of The Pharmaceutical Address Location Licence No. Present StatusAnamika SahaPas encore d'évaluation
- Module 1 - IntroductionDocument30 pagesModule 1 - Introductionpsychopharmacology100% (2)
- Fda'S Question-Based Review (QBR) : A Risk-Based Pharmaceutical Quality Assessment ToolDocument50 pagesFda'S Question-Based Review (QBR) : A Risk-Based Pharmaceutical Quality Assessment Toollalooprasad15Pas encore d'évaluation
- Pharmaceutical Jurisprudence NotesDocument34 pagesPharmaceutical Jurisprudence NotesSachin NagarPas encore d'évaluation
- Australian PTSD medication guidelinesDocument6 pagesAustralian PTSD medication guidelinesDaniel MartinezPas encore d'évaluation
- Valium Drug AnalysisDocument1 pageValium Drug AnalysisFerdinand Sherwin MorataPas encore d'évaluation
- Peform Calculations ActivityDocument6 pagesPeform Calculations ActivitySher RylPas encore d'évaluation
- Dosage Handouts 2020 2021Document16 pagesDosage Handouts 2020 2021chrystan maconPas encore d'évaluation
- Lactulose Drug StudyDocument4 pagesLactulose Drug StudyAgronaSlaughterPas encore d'évaluation
- Pre-Course MCQ ..................................Document1 pagePre-Course MCQ ..................................Arslan SiddiquiPas encore d'évaluation
- Savovent Company ProfileDocument8 pagesSavovent Company Profilemehta hemantPas encore d'évaluation
- OTCtxDocument3 pagesOTCtxlosangelesPas encore d'évaluation
- Major Depressive Disorder: By: YOHANES AYELE, M.Pharm, Lecturer, Harar Health Science CollegeDocument48 pagesMajor Depressive Disorder: By: YOHANES AYELE, M.Pharm, Lecturer, Harar Health Science Collegehab lemPas encore d'évaluation
- Mapeh Ikatlong Markahan: Edukasyong PangkalusuganDocument50 pagesMapeh Ikatlong Markahan: Edukasyong PangkalusuganCherilyn AbbangPas encore d'évaluation
- Pharma Notes 1Document9 pagesPharma Notes 1Mayya FirdousPas encore d'évaluation
- Pharmaceutical AnalysisDocument4 pagesPharmaceutical AnalysisYuri DryzgaPas encore d'évaluation
- DPRI 2018 Drug Price Reference Index UpdateDocument34 pagesDPRI 2018 Drug Price Reference Index UpdateShaenie Lou Gatillo67% (3)
- Gynisol SyrupDocument2 pagesGynisol Syruphk_scribdPas encore d'évaluation
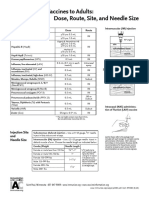
- Administering Vaccines To Adults: Dose, Route, Site, and Needle SizeDocument1 pageAdministering Vaccines To Adults: Dose, Route, Site, and Needle SizeAkashPas encore d'évaluation
- Ncm-106-Nursing-Process - Part3w1Document5 pagesNcm-106-Nursing-Process - Part3w1Marielle ChuaPas encore d'évaluation
- Formulari Farmacologic CFTDocument177 pagesFormulari Farmacologic CFTFernando MarquesPas encore d'évaluation
- Clarithromycin 2010 11 45 PdARDocument29 pagesClarithromycin 2010 11 45 PdARswabrijPas encore d'évaluation
- Tramadol + ParacetamolDocument4 pagesTramadol + ParacetamolFaye Andrea Francisco100% (2)
- ACLS Review TestDocument5 pagesACLS Review Testtostc60% (5)
- REPORT Mandela Kibiriti's ACLS scoresDocument2 pagesREPORT Mandela Kibiriti's ACLS scoresMandela KibiritiPas encore d'évaluation