Vous aimerez peut-être aussi
- Nursing As A Prof, HistoryDocument51 pagesNursing As A Prof, Historymags_abad09Pas encore d'évaluation
- The Impact of Emerging Technology On Nursing Care: Warp Speed AheadDocument16 pagesThe Impact of Emerging Technology On Nursing Care: Warp Speed Aheadphoenix180Pas encore d'évaluation
- Trends in NursingDocument8 pagesTrends in NursingVjs MrunaliniPas encore d'évaluation
- 07 Nurse-Patient Ratios As A Patient Safety Strategy PDFDocument7 pages07 Nurse-Patient Ratios As A Patient Safety Strategy PDFAmanda DavisPas encore d'évaluation
- Nursing As An Art Nursing As An Art Nursing As An Art Nursing As An ArtDocument14 pagesNursing As An Art Nursing As An Art Nursing As An Art Nursing As An Artraj100% (3)
- The Future of Nursing EducationDocument10 pagesThe Future of Nursing EducationAimee GutierrezPas encore d'évaluation
- The Analysis of Nurse Compliance in Documenting of Nursing Care in Islamic Hospital PalembangDocument11 pagesThe Analysis of Nurse Compliance in Documenting of Nursing Care in Islamic Hospital PalembangInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Orem's Self-Care Deficit TheoryDocument6 pagesOrem's Self-Care Deficit TheoryMary ShiksPas encore d'évaluation
- UnderstaffingDocument13 pagesUnderstaffingIrish Docoy PatesPas encore d'évaluation
- The Effect of Nurse Staffing On Patient-Safety Outcomes A Cross-Sectional SurveyDocument9 pagesThe Effect of Nurse Staffing On Patient-Safety Outcomes A Cross-Sectional SurveyLuoya houPas encore d'évaluation
- Summary On Evidence Based PracticeDocument1 pageSummary On Evidence Based Practiceteena17Pas encore d'évaluation
- History of NursingDocument8 pagesHistory of NursingNazareth Narisma PatindolPas encore d'évaluation
- Ethical Issues in NursingDocument30 pagesEthical Issues in NursingUpendra Yadav100% (2)
- Nursing in 21st CenturyDocument41 pagesNursing in 21st CenturyCarissa De Luzuriaga-Balaria0% (2)
- Patterns of Knowing EssayDocument6 pagesPatterns of Knowing Essayapi-282992446100% (2)
- Nurse Case StudyDocument6 pagesNurse Case Studyprateeksha16Pas encore d'évaluation
- Research NursingDocument20 pagesResearch NursingMimi Lizada BhattiPas encore d'évaluation
- Florence NightingaleDocument18 pagesFlorence NightingaleCarolina Alejandra Hernández GálvezPas encore d'évaluation
- Unit 2 Evidence Based Nursing PracticeDocument94 pagesUnit 2 Evidence Based Nursing Practicenoo.wann100% (2)
- PAPER 3 Nursing PhenomenonDocument7 pagesPAPER 3 Nursing PhenomenonMhel Es QuiadPas encore d'évaluation
- Level of Knowledge and Attitude Among Nursing Students Toward Patient Safety and Medical ErrorsDocument125 pagesLevel of Knowledge and Attitude Among Nursing Students Toward Patient Safety and Medical ErrorshanadiPas encore d'évaluation
- Autism, It Is Discussed Why People Started Believing That Vaccines Cause Autism. There Was ADocument8 pagesAutism, It Is Discussed Why People Started Believing That Vaccines Cause Autism. There Was Aapi-301643808Pas encore d'évaluation
- Current Trends in Nursing EducaionDocument14 pagesCurrent Trends in Nursing EducaionArchana SahuPas encore d'évaluation
- Analyse Nursing Data PDFDocument22 pagesAnalyse Nursing Data PDFRika FatmadonaPas encore d'évaluation
- Case Study CovidDocument6 pagesCase Study CovidAngel Faith TirolPas encore d'évaluation
- Perceived Safety Culture of Healthcare Providers in Hospitals in The PhilippinesDocument14 pagesPerceived Safety Culture of Healthcare Providers in Hospitals in The PhilippinesRhod Bernaldez EstaPas encore d'évaluation
- Nursing ImageDocument10 pagesNursing Imageapi-392400343Pas encore d'évaluation
- PJN Jan June 2021 Final Version CompleteDocument130 pagesPJN Jan June 2021 Final Version CompleteJohn Vincent LacuestaPas encore d'évaluation
- Scope of NursingDocument27 pagesScope of NursingBlanche Gonzalez100% (2)
- Evidence Based Practice in NursingDocument3 pagesEvidence Based Practice in NursingThrift Advisory100% (2)
- Lifelong Learning TheoryDocument21 pagesLifelong Learning TheoryXieng TiocoPas encore d'évaluation
- Ethical PrinciplesDocument6 pagesEthical PrinciplesSammy ChegePas encore d'évaluation
- ICU Admission, Discharge, and Triage GuidelinesDocument9 pagesICU Admission, Discharge, and Triage Guidelinesugi 23Pas encore d'évaluation
- Ethical CompetenceDocument28 pagesEthical CompetenceRysanPas encore d'évaluation
- Caring in NursingDocument60 pagesCaring in NursingChadrie SanchezPas encore d'évaluation
- Ethical Dilemmas Experienced by Nurses in Providing Care For Critically Ill Patients in Intensive Care Units, Medan, IndonesiaDocument9 pagesEthical Dilemmas Experienced by Nurses in Providing Care For Critically Ill Patients in Intensive Care Units, Medan, Indonesiaravibunga4489Pas encore d'évaluation
- Nurse ManagerDocument10 pagesNurse Managerapi-282133920100% (1)
- Thesis Male in NursingDocument64 pagesThesis Male in Nursingljago278512Pas encore d'évaluation
- The Lived Experience of NursesDocument161 pagesThe Lived Experience of NursesGermán AchuryPas encore d'évaluation
- Rawls' Theory of JusticeDocument13 pagesRawls' Theory of JusticeLarry MagallanoPas encore d'évaluation
- Journal 1 - Technology in Nursing - FinalDocument47 pagesJournal 1 - Technology in Nursing - FinalEmilio Antang JrPas encore d'évaluation
- Work-Related Stress in NursingDocument49 pagesWork-Related Stress in Nursinga_l_y_nPas encore d'évaluation
- Nursing DefinitionDocument30 pagesNursing Definitionaibuty100% (2)
- Human To Human Relationship ModelDocument4 pagesHuman To Human Relationship Modelrj carpsonPas encore d'évaluation
- Integrative Literature ReviewDocument23 pagesIntegrative Literature Reviewapi-428103455100% (1)
- Hospital Management Services, Inc - Medical Center Manila, Petitioner, vs. EmployeesDocument2 pagesHospital Management Services, Inc - Medical Center Manila, Petitioner, vs. EmployeesPrhyllePas encore d'évaluation
- Role Development AssignmentDocument9 pagesRole Development AssignmentElizabeth HoPas encore d'évaluation
- Nursing Theory PaperDocument5 pagesNursing Theory Paperapi-268670617Pas encore d'évaluation
- The Future of Nursing Service RegulationDocument81 pagesThe Future of Nursing Service RegulationthatiePas encore d'évaluation
- Nurses' Job Burnout and Job Satisfaction During The COVID-19 Pandemic in The PhilippinesDocument14 pagesNurses' Job Burnout and Job Satisfaction During The COVID-19 Pandemic in The PhilippinesShan AlejosPas encore d'évaluation
- Nursing TheoristsDocument18 pagesNursing TheoristsDanielle Elizabeth Andres100% (1)
- Global Trends and Issues in NursingDocument27 pagesGlobal Trends and Issues in NursingDolly Jiljith100% (1)
- Fields of Specialization in NursingDocument6 pagesFields of Specialization in NursingBella IsananPas encore d'évaluation
- Quantitative Research DesignDocument19 pagesQuantitative Research DesignAli Ahmed GhouriPas encore d'évaluation
- Huacasi White Paper WeeblyDocument11 pagesHuacasi White Paper Weeblyapi-397532577Pas encore d'évaluation
- Essential Iii-2Document12 pagesEssential Iii-2api-318152697Pas encore d'évaluation
- Lauren Vandaniker Technology Impact On Nursing PracticeDocument19 pagesLauren Vandaniker Technology Impact On Nursing PracticeAllysaPas encore d'évaluation
- Removal of Sharp Object Patient SaftyDocument6 pagesRemoval of Sharp Object Patient SaftyAlibaba AlihaihaiPas encore d'évaluation
- Alarm Safety Anf FatigueDocument16 pagesAlarm Safety Anf FatigueRaquel Olivares SanchezPas encore d'évaluation
- WFCCN Chapter 4 Safety-and-Quality-in-the-ICU 2nd EditionDocument13 pagesWFCCN Chapter 4 Safety-and-Quality-in-the-ICU 2nd EditionJuan Carlos Mora TorresPas encore d'évaluation
- Cee 2005 - 06Document129 pagesCee 2005 - 06iloveeggxPPas encore d'évaluation
- Gerin Bagaslino - 52417512Document13 pagesGerin Bagaslino - 52417512Gerin BagaslinoPas encore d'évaluation
- Fichas Slate HoneywellDocument1 pageFichas Slate HoneywellING CARLOS RAMOSPas encore d'évaluation
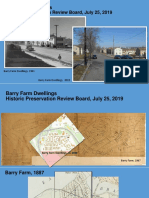
- Barry Farm Powerpoint SlidesDocument33 pagesBarry Farm Powerpoint SlidessarahPas encore d'évaluation
- Augmented FeedbackDocument54 pagesAugmented FeedbackAhmad KhuwarizmyPas encore d'évaluation
- M4-Lesson Transitional SignalDocument50 pagesM4-Lesson Transitional SignalJeneros PartosPas encore d'évaluation
- JurnalDocument24 pagesJurnaltsania rahmaPas encore d'évaluation
- DBR G+24 Building ProjectDocument28 pagesDBR G+24 Building ProjectShobhit Mohta100% (1)
- BharathDocument2 pagesBharathbharath kumarPas encore d'évaluation
- Affective DomainDocument3 pagesAffective DomainJm Enriquez Dela Cruz50% (2)
- Project PlanDocument8 pagesProject PlanRodsheen100% (1)
- Specification of SGP InterlayerDocument3 pagesSpecification of SGP InterlayerHAN HANPas encore d'évaluation
- Potential Application of Orange Peel (OP) As An Eco-Friendly Adsorbent For Textile Dyeing EffluentsDocument13 pagesPotential Application of Orange Peel (OP) As An Eco-Friendly Adsorbent For Textile Dyeing EffluentsAnoif Naputo AidnamPas encore d'évaluation
- Morning Report: Supervisor: Dr. H. Doddy Ak., Spog (K)Document10 pagesMorning Report: Supervisor: Dr. H. Doddy Ak., Spog (K)vika handayaniPas encore d'évaluation
- Computer Graphics Question For Final ExamDocument3 pagesComputer Graphics Question For Final ExamMd Rifat BhuiyanPas encore d'évaluation
- Control Panel Manual 1v4Document52 pagesControl Panel Manual 1v4Gustavo HidalgoPas encore d'évaluation
- IBRO News 2004Document8 pagesIBRO News 2004International Brain Research Organization100% (1)
- Tips Experiments With MatlabDocument190 pagesTips Experiments With MatlabVishalPas encore d'évaluation
- Cultural GlobalizationDocument16 pagesCultural Globalizationee0785Pas encore d'évaluation
- Internship Report On Service IndustryDocument50 pagesInternship Report On Service Industrybbaahmad89Pas encore d'évaluation
- Gender InequalityDocument9 pagesGender InequalityRhzPas encore d'évaluation
- (Herbert Kitschelt, Steven I. Wilkinson) Patrons, PDFDocument387 pages(Herbert Kitschelt, Steven I. Wilkinson) Patrons, PDFClemente Tomás Sánchez BarjaPas encore d'évaluation
- D027B OmronDocument141 pagesD027B OmronirfanWPKPas encore d'évaluation
- Multithreading AlgorithmsDocument36 pagesMultithreading AlgorithmsAsna TariqPas encore d'évaluation
- Network Management Systems 10CS834 PDFDocument113 pagesNetwork Management Systems 10CS834 PDFSarfraz AhmedPas encore d'évaluation
- Spinning CalculationDocument178 pagesSpinning Calculationamboklate69% (16)
- Sop For RetailDocument13 pagesSop For Retailkarthika suresh100% (6)
- PERFORM Toolkit 3 1 Release Notes 1.0 OnlinePDFDocument18 pagesPERFORM Toolkit 3 1 Release Notes 1.0 OnlinePDFJose HugoPas encore d'évaluation
- The Doppler EffectLDocument2 pagesThe Doppler EffectLintan100% (1)
- The Structure of Deception: Validation of The Lying Profile QuestionnaireDocument16 pagesThe Structure of Deception: Validation of The Lying Profile QuestionnaireNancy DrewPas encore d'évaluation