Vous aimerez peut-être aussi
- Presentation 513Document16 pagesPresentation 513api-284092317Pas encore d'évaluation
- Clinical SitesDocument1 pageClinical Sitesapi-284092317Pas encore d'évaluation
- Womens Health 650Document11 pagesWomens Health 650api-285177380Pas encore d'évaluation
- Nutrition and StressDocument38 pagesNutrition and Stressapi-284092317Pas encore d'évaluation
- Obesity Presentation-640Document12 pagesObesity Presentation-640api-284092317Pas encore d'évaluation
- Propranolol 1 PresentationDocument17 pagesPropranolol 1 Presentationapi-284092317100% (1)
- Presentation 660Document11 pagesPresentation 660api-284092317Pas encore d'évaluation
- Presentation 520Document10 pagesPresentation 520api-284092317Pas encore d'évaluation
- Theory Presentation-620Document13 pagesTheory Presentation-620api-284092317Pas encore d'évaluation
- Research Theory Paper - 620Document6 pagesResearch Theory Paper - 620api-284092317Pas encore d'évaluation
- Family Theory Presentation-512Document6 pagesFamily Theory Presentation-512api-284092317Pas encore d'évaluation
- Theory Paper-620Document7 pagesTheory Paper-620api-284092317Pas encore d'évaluation
- Presentation-Ethics - 500Document17 pagesPresentation-Ethics - 500api-284092317Pas encore d'évaluation
- Non-Thesis Paper-513Document38 pagesNon-Thesis Paper-513api-284092317100% (1)
- Scholarly Paper - Nurs-660Document13 pagesScholarly Paper - Nurs-660api-284092317Pas encore d'évaluation
- Professional Paper 505Document10 pagesProfessional Paper 505api-284092317Pas encore d'évaluation
- Tuskegee Study Paper - 500Document19 pagesTuskegee Study Paper - 500api-284092317Pas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5782)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Disc Plow SpecificationsDocument9 pagesDisc Plow SpecificationsJosé Inés Bazán Mota100% (1)
- L1 Security PrinciplesDocument18 pagesL1 Security PrinciplesJayz JoePas encore d'évaluation
- Environment - Parallel Session - Jo Rowena GarciaDocument26 pagesEnvironment - Parallel Session - Jo Rowena GarciaAsian Development Bank ConferencesPas encore d'évaluation
- Einstein & Inconsistency in General Relativity, by C. Y. LoDocument12 pagesEinstein & Inconsistency in General Relativity, by C. Y. Loicar1997100% (1)
- Preparing Your Tracks For Mixing - SoundBetterDocument5 pagesPreparing Your Tracks For Mixing - SoundBetterEmmanuel TuffetPas encore d'évaluation
- Songs For The Deaf: Parental Advisory EdDocument5 pagesSongs For The Deaf: Parental Advisory EdTinta CafePas encore d'évaluation
- 2023 Imec Wind Symphony ProgramDocument16 pages2023 Imec Wind Symphony Programapi-583612673Pas encore d'évaluation
- Week 1 - Topic: Chapter 2: The Foreign Exchange Market 21 March 2021Document36 pagesWeek 1 - Topic: Chapter 2: The Foreign Exchange Market 21 March 2021Jenita singhPas encore d'évaluation
- 2015 Quikrete Product Guide PDFDocument28 pages2015 Quikrete Product Guide PDFTushar PatelPas encore d'évaluation
- Inclusion/Exclusion PrincipleDocument6 pagesInclusion/Exclusion Principlekeelia1saPas encore d'évaluation
- 4024 w13 QP 11 PDFDocument20 pages4024 w13 QP 11 PDFChristine SetiawanPas encore d'évaluation
- Reliability Centered Maintenance ExplainationDocument6 pagesReliability Centered Maintenance Explainationambuenaflor100% (1)
- Vanguardia's Online Review Program: Genito-Urinary Tract FunctionDocument8 pagesVanguardia's Online Review Program: Genito-Urinary Tract FunctionBobet ReñaPas encore d'évaluation
- Machine Learning NNDocument16 pagesMachine Learning NNMegha100% (1)
- Thomas McPherson Brown MD Treatment of Rheumatoid DiseaseDocument29 pagesThomas McPherson Brown MD Treatment of Rheumatoid DiseaseLidia Lidia100% (1)
- CAM/CIM Process and NC Part Programming FundamentalsDocument16 pagesCAM/CIM Process and NC Part Programming FundamentalsRakhi Mol BVPas encore d'évaluation
- El 114 The-Adventures-of-Tom-Sawyer-by-Mark-TwainDocument11 pagesEl 114 The-Adventures-of-Tom-Sawyer-by-Mark-TwainGhreniel V. Benecito100% (1)
- Tips For A Successful Approval of A Fire Alarm SystemDocument9 pagesTips For A Successful Approval of A Fire Alarm SystemradusettPas encore d'évaluation
- Lectures SSY1352019Document307 pagesLectures SSY1352019S Awais Ahmed100% (2)
- Power One Model SLI-48-115 Data SheetDocument5 pagesPower One Model SLI-48-115 Data SheetshartsellPas encore d'évaluation
- Nano-C ENDocument1 pageNano-C ENMartín CoronelPas encore d'évaluation
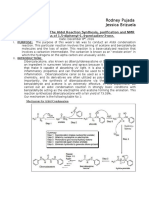
- LAB REPORT 7 Aldol Reaction Synthesis 1 5 Diphenyl 1 4 Pentadien 3 OneDocument6 pagesLAB REPORT 7 Aldol Reaction Synthesis 1 5 Diphenyl 1 4 Pentadien 3 OneChimiste ChimistePas encore d'évaluation
- Zinkgruvan Suecia Polimetálico TechRep - 2017Document178 pagesZinkgruvan Suecia Polimetálico TechRep - 2017manudemPas encore d'évaluation
- European Summary Report On CHP Support SchemesDocument33 pagesEuropean Summary Report On CHP Support SchemesioanitescumihaiPas encore d'évaluation
- Autism and Autism Spectrum Disorder Medical Hypothesis For Parasites Influencing AutismDocument3 pagesAutism and Autism Spectrum Disorder Medical Hypothesis For Parasites Influencing AutismCATHYPas encore d'évaluation
- School Form 1 SF 1 10Document6 pagesSchool Form 1 SF 1 10ALEX SARAOSOSPas encore d'évaluation
- Proposal Format:: Project Title: "Document4 pagesProposal Format:: Project Title: "wondi BETPas encore d'évaluation
- EnglishDocument19 pagesEnglishAliPas encore d'évaluation
- Legal CapacityDocument7 pagesLegal CapacityAreej UmerPas encore d'évaluation
- The Archaeology of Maritime Landscapes 2011Document363 pagesThe Archaeology of Maritime Landscapes 2011Adriana BernalPas encore d'évaluation