Vous aimerez peut-être aussi
- Cleft Lip and Cleft PalateDocument8 pagesCleft Lip and Cleft PalateRAJU33% (3)
- Cleft Lip and Cleft PalateDocument16 pagesCleft Lip and Cleft Palatemacuka08100% (3)
- Cleft Lip and PalateDocument25 pagesCleft Lip and PalateRahul Dhaker100% (1)
- Cleft Lip and PalateDocument18 pagesCleft Lip and Palateicywitch100% (1)
- Cleft Lip And Palate, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandCleft Lip And Palate, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÉvaluation : 4.5 sur 5 étoiles4.5/5 (3)
- Cleft Lip PalateDocument37 pagesCleft Lip PalateMuhammad Hamid Muktashim100% (1)
- Child - Cleft PalateDocument5 pagesChild - Cleft PalateMelanie Anne Montecillo Aringay100% (3)
- Cleft Palate: Wan Khadijah Wan Yusoff Noor Afika Binti AzriDocument91 pagesCleft Palate: Wan Khadijah Wan Yusoff Noor Afika Binti AzriWOne WannPas encore d'évaluation
- Palatoplasty Case StudyDocument26 pagesPalatoplasty Case StudySometwo C. Hangal100% (1)
- Case Study Cleft LipDocument55 pagesCase Study Cleft LipJaya Prabha50% (10)
- Tracheo-Oesophageal FistulaDocument19 pagesTracheo-Oesophageal Fistularajan kumar100% (3)
- IUGRDocument11 pagesIUGRAnastasiafynnPas encore d'évaluation
- Group 11 Cleft Lip and Cleft Palate Case Study N2BDocument46 pagesGroup 11 Cleft Lip and Cleft Palate Case Study N2BLerma PagcaliwanganPas encore d'évaluation
- Craniotomy Case StudyDocument14 pagesCraniotomy Case StudyHoney Semafranca PlatolonPas encore d'évaluation
- Pediatric Ist SeminarDocument21 pagesPediatric Ist SeminarAsha jiluPas encore d'évaluation
- CcroupDocument53 pagesCcroupOlivia BernadiPas encore d'évaluation
- Nursing Process of PneumoniaDocument5 pagesNursing Process of Pneumoniatin2x061275% (8)
- Care PlanDocument4 pagesCare PlangopscharanPas encore d'évaluation
- Family Case Study For HydrocephalusDocument9 pagesFamily Case Study For HydrocephalusjaegergranPas encore d'évaluation
- Patient Scenario, Chapter 45, Nursing Care of A Family When A Child Has A Gastrointestinal DisorderDocument93 pagesPatient Scenario, Chapter 45, Nursing Care of A Family When A Child Has A Gastrointestinal DisorderDay MedsPas encore d'évaluation
- TerminologyDocument38 pagesTerminologypandem soniyaPas encore d'évaluation
- Anatomy &physiology JaundiceDocument2 pagesAnatomy &physiology JaundiceHCX dghhqPas encore d'évaluation
- MSN Ii - 24.6.2020 An-Tonsillitis and AdenoiditisDocument41 pagesMSN Ii - 24.6.2020 An-Tonsillitis and AdenoiditisYAMINIPRIYANPas encore d'évaluation
- Physiological Changes During Pregnancy: Presented By: Ms. Vruti PatelDocument44 pagesPhysiological Changes During Pregnancy: Presented By: Ms. Vruti PatelSANJEEV KUMARPas encore d'évaluation
- Case Studybleeding Biliary AtresiaDocument13 pagesCase Studybleeding Biliary Atresialawrence tayamPas encore d'évaluation
- Case Presentation HydrocephalusDocument48 pagesCase Presentation HydrocephalusSu Osman50% (2)
- Pyloric StenosisDocument3 pagesPyloric Stenosismagisasamundo100% (1)
- Congenital Diaphragmatic HerniaDocument21 pagesCongenital Diaphragmatic HerniaJennifer Dixon100% (1)
- Oesophageal Atresia by GabriellaDocument7 pagesOesophageal Atresia by GabriellaGabriellePas encore d'évaluation
- What Is Retained PlacentaDocument7 pagesWhat Is Retained PlacentaA Xiao Yhing TrancoPas encore d'évaluation
- A Case Study About Cleft Lip and Cleft PalateDocument12 pagesA Case Study About Cleft Lip and Cleft PalateMaegan Pearl83% (6)
- Broncho PneumoniaDocument23 pagesBroncho Pneumoniaanon-84769398% (43)
- Esophageal ObstructionDocument18 pagesEsophageal ObstructionArun Murali50% (2)
- Asphyxia NeonatorumDocument29 pagesAsphyxia Neonatorummamaalyssa100% (1)
- Hypospadias and Epispadias 1Document35 pagesHypospadias and Epispadias 1Corey100% (1)
- Care of HemophiliaDocument7 pagesCare of HemophiliaBasant karn100% (4)
- Aetiology Heart Diasease in Children May Be Congenital or AcquiredDocument23 pagesAetiology Heart Diasease in Children May Be Congenital or AcquiredkasondaPas encore d'évaluation
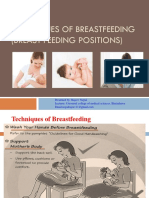
- Technique of Breast Feeding (Position of Breast Feeding)Document17 pagesTechnique of Breast Feeding (Position of Breast Feeding)Rajeev NepalPas encore d'évaluation
- EpisiotomyDocument18 pagesEpisiotomyAnnapurna DangetiPas encore d'évaluation
- Hookworm Diseases: (Ancylostomiasis /Miner'S Disease/Egyptian Chlorisis)Document21 pagesHookworm Diseases: (Ancylostomiasis /Miner'S Disease/Egyptian Chlorisis)Mel Izhra N. Margate100% (1)
- PP Insect Bite 2007 (Print)Document16 pagesPP Insect Bite 2007 (Print)Ali RumiPas encore d'évaluation
- Cephalopelvic DisproportionDocument3 pagesCephalopelvic DisproportionAira MiyaPas encore d'évaluation
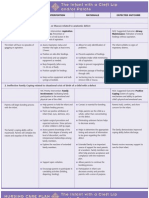
- NCP Priority 1 Assessment Diagnosis Planning Intervention Rationale EvaluationDocument5 pagesNCP Priority 1 Assessment Diagnosis Planning Intervention Rationale EvaluationDenice100% (1)
- Cleft Lip and Palate PDFDocument52 pagesCleft Lip and Palate PDFSylvia Anggraeni100% (2)
- NCM - Pregancy Induced HypertensionDocument5 pagesNCM - Pregancy Induced HypertensionZam PamatePas encore d'évaluation
- DEFINITION: Abortion Is The Expulsion or Extraction From Its MotherDocument10 pagesDEFINITION: Abortion Is The Expulsion or Extraction From Its MothermOHAN.SPas encore d'évaluation
- Intrauterine Growth RestrictionDocument21 pagesIntrauterine Growth Restrictionمصطفى محمدPas encore d'évaluation
- Presentation On Renal CalculiDocument16 pagesPresentation On Renal CalculiSangay CheshirePas encore d'évaluation
- Newborn AssessmentDocument9 pagesNewborn Assessmentapi-237668254Pas encore d'évaluation
- Acute Gastroenteritis Case StudyDocument20 pagesAcute Gastroenteritis Case StudyJohn Carlo Kimura Rabanes100% (1)
- Cleft Lip and Palate New ApproachDocument115 pagesCleft Lip and Palate New ApproachsoorajPas encore d'évaluation
- Case Study of HypospadiaDocument19 pagesCase Study of Hypospadialicservernoida100% (2)
- Assignment On Wound HealingDocument5 pagesAssignment On Wound HealingShamaPas encore d'évaluation
- Cleft Lip and Palate - PPT - OrthodonticsDocument46 pagesCleft Lip and Palate - PPT - OrthodonticsDr.Neethu Salam100% (3)
- Nursing Diagnosis For AppendicitisDocument1 pageNursing Diagnosis For AppendicitisTweenie DalumpinesPas encore d'évaluation
- Cleft Lip and Cleft PalateDocument22 pagesCleft Lip and Cleft PalateOm VaishNav0% (1)
- Cleft Palate and Cleft Lip IntroductionDocument3 pagesCleft Palate and Cleft Lip IntroductionCLaui SagibalPas encore d'évaluation
- Content Congenital DisorderDocument20 pagesContent Congenital DisorderKaka SalvatorePas encore d'évaluation
- Cleft Lip and Cleft PalateDocument16 pagesCleft Lip and Cleft PalateIsmail LubisPas encore d'évaluation
- Cleft Lip and Cleft PalateDocument6 pagesCleft Lip and Cleft PalatekrishnasreePas encore d'évaluation
- Classical Five-Element Acupuncture: Two More Powerful Treatment StrategiesDocument10 pagesClassical Five-Element Acupuncture: Two More Powerful Treatment StrategiesAPas encore d'évaluation
- Lenin PostmortemDocument6 pagesLenin Postmortemapi-196020598Pas encore d'évaluation
- Antibiotic Susceptibility of Bacterial Isolates FRDocument8 pagesAntibiotic Susceptibility of Bacterial Isolates FRkaren leePas encore d'évaluation
- Actual 2Document1 pageActual 2joaquin trinidadPas encore d'évaluation
- Original PDF Complementary and Alternative Therapies For Nursing Practice 5th PDFDocument41 pagesOriginal PDF Complementary and Alternative Therapies For Nursing Practice 5th PDFpaul.shropshire768100% (37)
- HERBALISTA First Aid Station HandoutDocument2 pagesHERBALISTA First Aid Station HandoutPhilip Scofield0% (1)
- Responsibilities of A CRADocument15 pagesResponsibilities of A CRAapi-3810976Pas encore d'évaluation
- Methods of EpidemiologyDocument28 pagesMethods of EpidemiologyAlice sylviya SamuelPas encore d'évaluation
- EARSS 2005 - tcm61-34899Document147 pagesEARSS 2005 - tcm61-34899api-3760696Pas encore d'évaluation
- Gestational Diabetes Mellitus Nursing Care PlanDocument1 pageGestational Diabetes Mellitus Nursing Care PlanASIS, MARK ANTHONY M.Pas encore d'évaluation
- Pre Transfusion TestingDocument57 pagesPre Transfusion TestingDominic Bernardo100% (4)
- Activity Design For Feeding Program (Repaired) 11Document5 pagesActivity Design For Feeding Program (Repaired) 11Cheryl PanolinoPas encore d'évaluation
- GSK ReportdDocument6 pagesGSK ReportdAsad MuhammadPas encore d'évaluation
- Crystalloids Versus Colloids Exploring.17Document14 pagesCrystalloids Versus Colloids Exploring.17Maria Siachoque JaraPas encore d'évaluation
- Salt and High Blood Pressure: Sailesh MOHAN and Norm R. C. CAMPBELLDocument11 pagesSalt and High Blood Pressure: Sailesh MOHAN and Norm R. C. CAMPBELLIndadul MozumdarPas encore d'évaluation
- Mental Health Case StudyDocument14 pagesMental Health Case Studyapi-592362133Pas encore d'évaluation
- MaretDocument132 pagesMarettipanoesaPas encore d'évaluation
- Drug Study Table OkDocument29 pagesDrug Study Table OkRifa'atul Mahmudah100% (1)
- Duke Anxiety-Depression Scale (DUKE-AD) : During The Past Week: How Much Trouble Have You Had WithDocument2 pagesDuke Anxiety-Depression Scale (DUKE-AD) : During The Past Week: How Much Trouble Have You Had WithvkPas encore d'évaluation
- Lichen Plan UsDocument26 pagesLichen Plan UsRebin AliPas encore d'évaluation
- AmazonDocument8 pagesAmazonKlaudia KałużnaPas encore d'évaluation
- Iasp Finalpreview - PHP Absnum 107579Document2 pagesIasp Finalpreview - PHP Absnum 107579eswar110582Pas encore d'évaluation
- Quirino Ave. Corner Roxas BLVD., Malate, ManilaDocument2 pagesQuirino Ave. Corner Roxas BLVD., Malate, ManilaChristian RoquePas encore d'évaluation
- Orthodontics-Gurkeerat Singh, 2nd EditionDocument704 pagesOrthodontics-Gurkeerat Singh, 2nd Editionkeralaapple85% (34)
- Diarrhea Case PresentationDocument20 pagesDiarrhea Case Presentationriya singh100% (8)
- Group (DSKTJP) Mini Project DPK20073Document11 pagesGroup (DSKTJP) Mini Project DPK20073Keshini RameshPas encore d'évaluation
- Altered Mental StateDocument2 pagesAltered Mental Stateizzati94Pas encore d'évaluation
- Nursing Leadership and Management Practice TestDocument1 pageNursing Leadership and Management Practice TestMikhaela GonzalesPas encore d'évaluation
- %pediatric TracheostomyDocument25 pages%pediatric TracheostomyFabian Camelo OtorrinoPas encore d'évaluation
- MCNDocument4 pagesMCNAijem RyanPas encore d'évaluation