Vous aimerez peut-être aussi
- Test Bank For Health and Physical Assessment in Nursing 4th Edition by FenskeDocument33 pagesTest Bank For Health and Physical Assessment in Nursing 4th Edition by FenskeHeriberto Murray100% (37)
- The Seal of Good Local Act of 2019: GovernanceDocument17 pagesThe Seal of Good Local Act of 2019: GovernanceRohaina Sapal100% (2)
- Public Health Nursing and The Disaster Management CycleDocument25 pagesPublic Health Nursing and The Disaster Management CycleLeadisti ArianiPas encore d'évaluation
- Tobacco Cessation PlanDocument11 pagesTobacco Cessation PlanEsteban García EcheverryPas encore d'évaluation
- Smoking Cessation ProgramDocument5 pagesSmoking Cessation ProgrampeterjongPas encore d'évaluation
- Making Connections Unit 2 PDFDocument54 pagesMaking Connections Unit 2 PDFDilraj0% (1)
- CE Winter Smoking CessationDocument7 pagesCE Winter Smoking CessationMiclăuș GeorgePas encore d'évaluation
- Ur 5 T TCXT OE55 YQIvf 5 OQD5 U U6 B PZPZY2 V AXH93 YRDocument12 pagesUr 5 T TCXT OE55 YQIvf 5 OQD5 U U6 B PZPZY2 V AXH93 YRkhayezulu032Pas encore d'évaluation
- Solutions of Negative ExternalitiesDocument6 pagesSolutions of Negative ExternalitiesnadiahPas encore d'évaluation
- Healthcare Professionals Health Systems HDocument2 pagesHealthcare Professionals Health Systems HARAFAT MIAHPas encore d'évaluation
- DH 402 TBDHU Presentation Smoking Cessation WorksheetDocument3 pagesDH 402 TBDHU Presentation Smoking Cessation Worksheetompatel.indPas encore d'évaluation
- 4 - Tobacco and Substance UseDocument20 pages4 - Tobacco and Substance UseCoral Srinivasa RamaluPas encore d'évaluation
- Healthy LivingDocument5 pagesHealthy Livingjamesrhylieabella6Pas encore d'évaluation
- Module 4. Ready To QuitDocument7 pagesModule 4. Ready To QuitMerville HCPas encore d'évaluation
- Smoking CessationDocument8 pagesSmoking CessationMary Jane MarcoPas encore d'évaluation
- Smoking Cessation Program: Dr. Rasha Salama PHD Community Medicine Suez Canal University EgyptDocument52 pagesSmoking Cessation Program: Dr. Rasha Salama PHD Community Medicine Suez Canal University EgyptTep TepPas encore d'évaluation
- Smoking CessationDocument4 pagesSmoking CessationAimee GutierrezPas encore d'évaluation
- Smoking Cessation Program: RationaleDocument5 pagesSmoking Cessation Program: RationaleJovic PocoPas encore d'évaluation
- Treating Tobacco Use and Dependence: Clinical Practice GuidelineDocument196 pagesTreating Tobacco Use and Dependence: Clinical Practice Guidelinesah770Pas encore d'évaluation
- Truth Initiative Statement On Harm Reduction FinalDocument13 pagesTruth Initiative Statement On Harm Reduction FinalBrent StaffordPas encore d'évaluation
- Tobacco Cessation Treatment PlanDocument7 pagesTobacco Cessation Treatment PlanyellowishmustardPas encore d'évaluation
- Behavioral Approaches To Smoking Cessation - UpToDateDocument23 pagesBehavioral Approaches To Smoking Cessation - UpToDatepablohbordaoPas encore d'évaluation
- Smoking Cessation: What Good Will Doctor's Advice Do?Document6 pagesSmoking Cessation: What Good Will Doctor's Advice Do?Getstop SmokingPas encore d'évaluation
- Carving Tobacco Cessation Out of Wellness:: Make A Real Impact On Tobacco Use in Your OrganizationDocument17 pagesCarving Tobacco Cessation Out of Wellness:: Make A Real Impact On Tobacco Use in Your OrganizationAnurag JainPas encore d'évaluation
- Smoking Cessation Guidelines: For Australian General PracticeDocument26 pagesSmoking Cessation Guidelines: For Australian General PracticePraveen KumarPas encore d'évaluation
- How To Encourage To Stop SmokingDocument12 pagesHow To Encourage To Stop SmokingSamPas encore d'évaluation
- Anne Buttigieg: Abutt01@um - Edu.mt Anne - Buttigieg@gov - MTDocument30 pagesAnne Buttigieg: Abutt01@um - Edu.mt Anne - Buttigieg@gov - MTTONY GO AWAYPas encore d'évaluation
- Tobacco Cessation, Why It Maters For EmployersDocument19 pagesTobacco Cessation, Why It Maters For EmployersIndonesia TobaccoPas encore d'évaluation
- Smoking Cessation Literature ReviewDocument8 pagesSmoking Cessation Literature Reviewafmzvaeeowzqyv100% (1)
- ALA Billing Guide 2021Document16 pagesALA Billing Guide 2021Libi FarrellPas encore d'évaluation
- Guidance On Brief Interventions and Referral For SmokingDocument36 pagesGuidance On Brief Interventions and Referral For Smokingmemad2022Pas encore d'évaluation
- Smoking Cheat SheetDocument8 pagesSmoking Cheat SheetMyra BuellaPas encore d'évaluation
- Fact Sheet Mental Illness and SmokingDocument4 pagesFact Sheet Mental Illness and SmokingTee R TaylorPas encore d'évaluation
- Effective Smoking CEssationDocument41 pagesEffective Smoking CEssationDhruva PatelPas encore d'évaluation
- Chapter 3 Behavioural and Advice Based Support For Smoking CessationDocument9 pagesChapter 3 Behavioural and Advice Based Support For Smoking CessationFoamm KitPas encore d'évaluation
- Smoking JournalDocument3 pagesSmoking Journaldamcon7Pas encore d'évaluation
- CP AssignmentDocument15 pagesCP AssignmentZahida BashirPas encore d'évaluation
- Global Tobacco EpidemicDocument100 pagesGlobal Tobacco EpidemicIndonesia TobaccoPas encore d'évaluation
- Ministry of Health & Family Welfare, Government of IndiaDocument6 pagesMinistry of Health & Family Welfare, Government of IndiarichakumariamityPas encore d'évaluation
- The SANE Smokefree KitDocument129 pagesThe SANE Smokefree KitSANE AustraliaPas encore d'évaluation
- Smoking CessationDocument4 pagesSmoking CessationEliana MuisPas encore d'évaluation
- 10' Smoking CessationDocument1 page10' Smoking CessationfabiandionisioPas encore d'évaluation
- Smoking HandoutDocument1 pageSmoking HandoutMac-Ross CordovaPas encore d'évaluation
- Arguments and Counter ArgumentsDocument38 pagesArguments and Counter ArgumentsmosmerahuPas encore d'évaluation
- Dapus Referat No.4Document7 pagesDapus Referat No.4Muhammad AkrimPas encore d'évaluation
- Art03 PDFDocument13 pagesArt03 PDFMauricio Alfredo Mardones SilvaPas encore d'évaluation
- Business Research On Consumer Buying Behavior After The Implementation of Sin Tax Law in The PhilippinesDocument41 pagesBusiness Research On Consumer Buying Behavior After The Implementation of Sin Tax Law in The PhilippinesMajoy Mendoza100% (2)
- Persuasive LetterDocument7 pagesPersuasive LetterRuby JosephPas encore d'évaluation
- Want To Be Hale and Strong Even at 80? Quit Smoking Now and Join The Smoking Cessation Program!Document3 pagesWant To Be Hale and Strong Even at 80? Quit Smoking Now and Join The Smoking Cessation Program!Mariah VivasPas encore d'évaluation
- Global Tobacco EpidemicDocument5 pagesGlobal Tobacco Epidemicsai vaibhavPas encore d'évaluation
- Module 5. Staying Quit or RelapseDocument5 pagesModule 5. Staying Quit or RelapseMerville HCPas encore d'évaluation
- Johnson & Johnson Case StudyDocument3 pagesJohnson & Johnson Case StudysulimayuPas encore d'évaluation
- You Can Quit Smoking: Consumer GuideDocument15 pagesYou Can Quit Smoking: Consumer GuideBrian HunzikerPas encore d'évaluation
- Quit SmokingDocument2 pagesQuit Smokingsummair showkatPas encore d'évaluation
- Strategies and Design of Hypnosis Intervention ForDocument26 pagesStrategies and Design of Hypnosis Intervention ForClaudia AranedaPas encore d'évaluation
- Stop Smoking: Proven Steps And Strategies To Make You Quit Smoking For GoodD'EverandStop Smoking: Proven Steps And Strategies To Make You Quit Smoking For GoodÉvaluation : 4 sur 5 étoiles4/5 (1)
- Effect of Smoking To TeenagersDocument7 pagesEffect of Smoking To TeenagersSiti Haridah AJPas encore d'évaluation
- D Grade Round 4 That+smokers+should+not+have+their+medical+treatments+subsidisedDocument1 pageD Grade Round 4 That+smokers+should+not+have+their+medical+treatments+subsidisedivan7tatPas encore d'évaluation
- Nursing Dissertation SmokingDocument8 pagesNursing Dissertation SmokingCustomPapersOnlineSingapore100% (1)
- Smoking Cessation Final FileDocument2 pagesSmoking Cessation Final Fileirene lumactodPas encore d'évaluation
- Treating Nicotine Dependence with Nitrous Oxide/Oxygen (PAN): A Manual for Health ProfessionalsD'EverandTreating Nicotine Dependence with Nitrous Oxide/Oxygen (PAN): A Manual for Health ProfessionalsPas encore d'évaluation
- Role of Hospital Pharmacist in Managment Smoking CessationDocument14 pagesRole of Hospital Pharmacist in Managment Smoking CessationMohammed HamdyPas encore d'évaluation
- Experts Call On WHO To Embrace E-Cigarettes As Tobacco Harm ReductionDocument7 pagesExperts Call On WHO To Embrace E-Cigarettes As Tobacco Harm ReductionJoan van DykPas encore d'évaluation
- Strategies For Breaking Free From Smoking, Vaping And Smokeless Tobacco - Based On The Teachings Of Dr. Andrew Huberman: Kicking The HabitD'EverandStrategies For Breaking Free From Smoking, Vaping And Smokeless Tobacco - Based On The Teachings Of Dr. Andrew Huberman: Kicking The HabitPas encore d'évaluation
- [Pediatrics, Child and Adolescent Health] Donald E. Greydanus, Dilip R. Patel, Ahsan Nazeer, Roger W. Appl - Behavioral Pediatrics_ Mental Health and Management (2022, Nova Science Publishers) - Libgen.liDocument352 pages[Pediatrics, Child and Adolescent Health] Donald E. Greydanus, Dilip R. Patel, Ahsan Nazeer, Roger W. Appl - Behavioral Pediatrics_ Mental Health and Management (2022, Nova Science Publishers) - Libgen.liDarrenDakaPas encore d'évaluation
- Chronic Kidney Disease Causes, Symptoms, Treatment, PreventionDocument7 pagesChronic Kidney Disease Causes, Symptoms, Treatment, PreventionNitaPas encore d'évaluation
- Concepts of Health and IllnessDocument35 pagesConcepts of Health and IllnessDominic SantosPas encore d'évaluation
- System Model-Betty Neuman: Objectives Ii. Central CoreDocument3 pagesSystem Model-Betty Neuman: Objectives Ii. Central CoreKrizzanne Flores100% (1)
- Lesson 2 - Global Health Initiatives 10Document23 pagesLesson 2 - Global Health Initiatives 10Margie SimoganPas encore d'évaluation
- Moph Annual Report 2017 Eng V3Document31 pagesMoph Annual Report 2017 Eng V3Diablo SinghPas encore d'évaluation
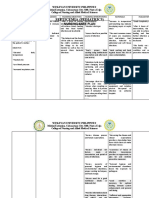
- Septicemia (Pediatrics) Nursing Care PlanDocument3 pagesSepticemia (Pediatrics) Nursing Care PlanMaybelyn Dela CruzPas encore d'évaluation
- Review Notes in PHCDocument130 pagesReview Notes in PHCJohn Michael Manlupig Pitoy100% (1)
- Body Mass Index and Body Composition Measures by Dual X-Ray Absorptiometry in Patients Aged 10 To 21 Years With Spinal Cord InjuryDocument8 pagesBody Mass Index and Body Composition Measures by Dual X-Ray Absorptiometry in Patients Aged 10 To 21 Years With Spinal Cord InjuryJoão Pedro PontesPas encore d'évaluation
- Lawa National High School First Quarter Spot TestDocument2 pagesLawa National High School First Quarter Spot TestRoderick Beltran LutangPas encore d'évaluation
- EpidemiologyDocument27 pagesEpidemiologyapi-343670182Pas encore d'évaluation
- CV Vivek Benegal 0610Document16 pagesCV Vivek Benegal 0610bhaskarsg0% (1)
- Nursing Care Plan: Risk For InfectionDocument3 pagesNursing Care Plan: Risk For Infectiongeorgeborja414726100% (3)
- An Overview of Community Health Nursing Practice in The PhilippinesDocument21 pagesAn Overview of Community Health Nursing Practice in The PhilippinesWilma BeraldePas encore d'évaluation
- Maguire2022 Article BehavioralTrainingAndPerformanDocument9 pagesMaguire2022 Article BehavioralTrainingAndPerformanZoha AliPas encore d'évaluation
- Introduction To Community B.SC Ii Yr CHNDocument77 pagesIntroduction To Community B.SC Ii Yr CHNJOSEPH IVO A. AGUINALDOPas encore d'évaluation
- Public Health Microbiology - 4th EdDocument39 pagesPublic Health Microbiology - 4th EdaphethuxolomPas encore d'évaluation
- Research Paper 2Document37 pagesResearch Paper 2api-628388847Pas encore d'évaluation
- Introduction To LM - Module 1, Week 1-1Document29 pagesIntroduction To LM - Module 1, Week 1-1OlayinkaPas encore d'évaluation
- Module 3 - Traditional Marketing - LectureDocument10 pagesModule 3 - Traditional Marketing - LectureMilan FantasyPas encore d'évaluation
- "Family Typology": in Partial Fulfillment of The Requirements in Community Organizing Participatory and Action ResearchDocument29 pages"Family Typology": in Partial Fulfillment of The Requirements in Community Organizing Participatory and Action Researchcalotz_chubie6891Pas encore d'évaluation
- Killiliisa StrategyDocument49 pagesKilliliisa StrategyNunatsiaqNewsPas encore d'évaluation
- Community & PHD - CurriculumDocument6 pagesCommunity & PHD - CurriculumManish AdhikariPas encore d'évaluation
- Community Health Nursing Lecture MODULE 2Document4 pagesCommunity Health Nursing Lecture MODULE 2Meryville JacildoPas encore d'évaluation
- Meinhardt WaterborneDiseaseDocument3 pagesMeinhardt WaterborneDiseaseਮਕੁਮਾਰPas encore d'évaluation
- 50 QuestionsDocument12 pages50 QuestionsDhon ProkopyoPas encore d'évaluation
































































![[Pediatrics, Child and Adolescent Health] Donald E. Greydanus, Dilip R. Patel, Ahsan Nazeer, Roger W. Appl - Behavioral Pediatrics_ Mental Health and Management (2022, Nova Science Publishers) - Libgen.li](https://imgv2-1-f.scribdassets.com/img/document/672408669/149x198/71304052a7/1710557812?v=1)