Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- All Vaccinees Are Requested To Bring Certificate of Dose-II From COWIN Portal Alongwith Registered Mobile Number Before Proceeding For VaccinationDocument7 pagesAll Vaccinees Are Requested To Bring Certificate of Dose-II From COWIN Portal Alongwith Registered Mobile Number Before Proceeding For VaccinationRakesh KumarPas encore d'évaluation
- Assignment 2 ME 326Document10 pagesAssignment 2 ME 326divided.symphonyPas encore d'évaluation
- The Ethics of CloningDocument5 pagesThe Ethics of CloningUpai MbembPas encore d'évaluation
- Ciac - HW Brochure Seer 16Document2 pagesCiac - HW Brochure Seer 16Tatiana DiazPas encore d'évaluation
- UNICEF Annual Report - Water 2018Document20 pagesUNICEF Annual Report - Water 2018Ross WeistrofferPas encore d'évaluation
- Apport D Un Fonds de Commerce en SocieteDocument28 pagesApport D Un Fonds de Commerce en SocieteJezebethPas encore d'évaluation
- Green Partnership of The Future: DieselfactsDocument12 pagesGreen Partnership of The Future: DieselfactsKamal WanniarachchiPas encore d'évaluation
- Akin To PityDocument356 pagesAkin To PityPaul StewartPas encore d'évaluation
- Esomeprazol Vs RabeprazolDocument7 pagesEsomeprazol Vs RabeprazolpabloPas encore d'évaluation
- Monitor Zoncare - PM-8000 ServicemanualDocument83 pagesMonitor Zoncare - PM-8000 Servicemanualwilmer100% (1)
- Dolor Postoperatorio y Efectos Secundarios de La Uvulo Palstia Con Radiofrecuencia en Roncopatia Primaria.Document5 pagesDolor Postoperatorio y Efectos Secundarios de La Uvulo Palstia Con Radiofrecuencia en Roncopatia Primaria.Alejandro RuizPas encore d'évaluation
- EML Prosedur ManualDocument1 019 pagesEML Prosedur Manualzrohim bapetenkfk2023Pas encore d'évaluation
- Phyilosophy of Midwifery Care 2Document13 pagesPhyilosophy of Midwifery Care 2Noella BezzinaPas encore d'évaluation
- Questions To Client On SAP HCMDocument19 pagesQuestions To Client On SAP HCMeurofighterPas encore d'évaluation
- Final Plant Diversity Lab ReportDocument6 pagesFinal Plant Diversity Lab Reportapi-508660724Pas encore d'évaluation
- Structral DatasheetDocument254 pagesStructral DatasheetdeepakPas encore d'évaluation
- Republic Act No. 10070Document3 pagesRepublic Act No. 10070Ganiela MCPas encore d'évaluation
- Level 9 - Unit 34Document7 pagesLevel 9 - Unit 34Javier RiquelmePas encore d'évaluation
- Lenovo TAB 2 A8-50: Hardware Maintenance ManualDocument69 pagesLenovo TAB 2 A8-50: Hardware Maintenance ManualGeorge KakoutPas encore d'évaluation
- EV-H-A1R 54C - M - EN - 2014 - D - Heat Detector SalwicoDocument2 pagesEV-H-A1R 54C - M - EN - 2014 - D - Heat Detector SalwicoCarolinaPas encore d'évaluation
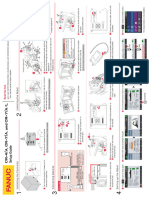
- CR-7iA CR-4iA Installation and Setup Guide (B-83774JA-1 01)Document1 pageCR-7iA CR-4iA Installation and Setup Guide (B-83774JA-1 01)lidiia.pavlkukPas encore d'évaluation
- 8582d Soldering Station English User GuideDocument9 pages8582d Soldering Station English User Guide1valdasPas encore d'évaluation
- Air Conditioning Is Inoperative, Fault Code 91eb11 or 91eb15 Is StoredDocument5 pagesAir Conditioning Is Inoperative, Fault Code 91eb11 or 91eb15 Is Storedwasim AiniaPas encore d'évaluation
- LR-360KAS-BROCHURE-LNG Sampling SystemsDocument4 pagesLR-360KAS-BROCHURE-LNG Sampling SystemsIdehen KelvinPas encore d'évaluation
- Vinegar Intake Reduces Body Weight Body Fat Mass and Serum Triglyceride Levels in Obese Japanese SubjectsDocument8 pagesVinegar Intake Reduces Body Weight Body Fat Mass and Serum Triglyceride Levels in Obese Japanese SubjectsZaphan ZaphanPas encore d'évaluation
- Retropharyngeal Abscess (RPA)Document15 pagesRetropharyngeal Abscess (RPA)Amri AshshiddieqPas encore d'évaluation
- Functional Capacity Evaluation: Occupational Therapy's Role inDocument2 pagesFunctional Capacity Evaluation: Occupational Therapy's Role inramesh babu100% (1)
- TG Chap. 10Document7 pagesTG Chap. 10Gissele AbolucionPas encore d'évaluation
- Report On Marketing of ArecanutDocument22 pagesReport On Marketing of ArecanutsivakkmPas encore d'évaluation
- Barangay Clearance SampleDocument1 pageBarangay Clearance SampleBarangay Onse Malaybalay100% (3)