Vous aimerez peut-être aussi
- EbpDocument44 pagesEbpapi-356127291Pas encore d'évaluation
- Cauti Prevention Qi ProjectDocument9 pagesCauti Prevention Qi Projectapi-596656815Pas encore d'évaluation
- Ebp Powerpoint PresentationDocument40 pagesEbp Powerpoint Presentationapi-383379774Pas encore d'évaluation
- Cauti Qi PosterDocument1 pageCauti Qi Posterapi-219780992Pas encore d'évaluation
- Reduce CAUTIs with Core Prevention StrategiesDocument32 pagesReduce CAUTIs with Core Prevention StrategiesArleen DevitaPas encore d'évaluation
- Qsen Project Urinary Catheter ComplicationsDocument18 pagesQsen Project Urinary Catheter Complicationsapi-316643564Pas encore d'évaluation
- Pressure Ulcer Risk Assessment The Braden Scale: Deepesh Bhardwaj Associate ProfessorDocument13 pagesPressure Ulcer Risk Assessment The Braden Scale: Deepesh Bhardwaj Associate ProfessorLaly ThomasPas encore d'évaluation
- Complications of Urinary Bladder Catheters and Preventive Strategies - UpToDateDocument8 pagesComplications of Urinary Bladder Catheters and Preventive Strategies - UpToDateJose Antonio Solis ChipaPas encore d'évaluation
- Bedside CommunicationDocument17 pagesBedside CommunicationY. Beatrice AbigailPas encore d'évaluation
- Bedsore TractionDocument8 pagesBedsore TractionDeevish N DinakarPas encore d'évaluation
- Wound Care: Presentation For ACC Lab March 22, 2006Document19 pagesWound Care: Presentation For ACC Lab March 22, 2006heka_amrongPas encore d'évaluation
- Prevent Pressure Ulcers with Proper Skin Care, Repositioning and Support SurfacesDocument6 pagesPrevent Pressure Ulcers with Proper Skin Care, Repositioning and Support SurfacesasuratosPas encore d'évaluation
- Prevalence of high-grade pressure ulcers reaches 4Document14 pagesPrevalence of high-grade pressure ulcers reaches 4Neneng WulandariPas encore d'évaluation
- Intravenous CannulationDocument9 pagesIntravenous CannulationjeorjPas encore d'évaluation
- Careplan 2 NSG 434 CCDocument8 pagesCareplan 2 NSG 434 CCapi-509642710Pas encore d'évaluation
- GROUP 4 (Myasthenia Gravis)Document53 pagesGROUP 4 (Myasthenia Gravis)gabrielle magdaraogPas encore d'évaluation
- Heparin Infusion Guideline PDFDocument3 pagesHeparin Infusion Guideline PDFbrigde_xPas encore d'évaluation
- RN Ward Manager RolesDocument21 pagesRN Ward Manager Rolesyenaj36Pas encore d'évaluation
- Standard EMDEX II SpecificationsDocument1 pageStandard EMDEX II SpecificationsxyzfieldPas encore d'évaluation
- Ccu NotesDocument76 pagesCcu NotesAr PeePas encore d'évaluation
- Nursing Shortage Final Revision 1Document13 pagesNursing Shortage Final Revision 1api-341876370Pas encore d'évaluation
- Data Analytics Final PresentationDocument11 pagesData Analytics Final Presentationapi-643967604Pas encore d'évaluation
- 08 Preventing In-Facility Pressure Ulcers As A Patient Safety StrategyDocument10 pages08 Preventing In-Facility Pressure Ulcers As A Patient Safety StrategyAmanda DavisPas encore d'évaluation
- Sample MealsDocument8 pagesSample MealsMarina_Abd_Rah_5529Pas encore d'évaluation
- Foley CathetersDocument13 pagesFoley Catheterslauramphs79Pas encore d'évaluation
- Groupd Ebp PresentationDocument38 pagesGroupd Ebp Presentationapi-384226081Pas encore d'évaluation
- Nurse-Directed Interventions To Reduce Catheter-Associated Urinary Tract InfectionsDocument10 pagesNurse-Directed Interventions To Reduce Catheter-Associated Urinary Tract InfectionsAngernani Trias WulandariPas encore d'évaluation
- University of Colorado NICHE Practice Survey SummaryDocument48 pagesUniversity of Colorado NICHE Practice Survey Summarybocah_britpopPas encore d'évaluation
- Catheter-Associated Urinary Tract InfectionsDocument20 pagesCatheter-Associated Urinary Tract Infectionsapi-315336673Pas encore d'évaluation
- Cauti PreventionDocument25 pagesCauti Preventionapi-340511634Pas encore d'évaluation
- Cauti Prevention - UpdatedDocument25 pagesCauti Prevention - Updatedapi-340518242Pas encore d'évaluation
- Cauti PreventionDocument25 pagesCauti Preventionapi-340154088Pas encore d'évaluation
- Nurse Driven Protocols ArticleDocument7 pagesNurse Driven Protocols ArticlePaolo VegaPas encore d'évaluation
- Implementing An Evidence-Based Practice Protocol For Prevention of Catheterized Associated Urinary Tract Infections in A Progressive Care UnitDocument9 pagesImplementing An Evidence-Based Practice Protocol For Prevention of Catheterized Associated Urinary Tract Infections in A Progressive Care UnitLina Mahayaty SembiringPas encore d'évaluation
- Pod Cast On Prevention of Catheter Associated Urinary Tract Infection 2Document12 pagesPod Cast On Prevention of Catheter Associated Urinary Tract Infection 2api-317345513Pas encore d'évaluation
- Final Quality Improvement PaperDocument8 pagesFinal Quality Improvement Paperapi-251822043Pas encore d'évaluation
- Cauti101 508Document40 pagesCauti101 508Yahia HassaanPas encore d'évaluation
- Nurs490 Cauti Safety Paper NeuburgDocument17 pagesNurs490 Cauti Safety Paper Neuburgapi-452041818100% (1)
- science: Auditing Urinary Catheter CareDocument7 pagesscience: Auditing Urinary Catheter CareNissa ErLinaPas encore d'évaluation
- Cduc Cwhi Jcas Rale Gnrs 586 Qi PresentationDocument11 pagesCduc Cwhi Jcas Rale Gnrs 586 Qi Presentationapi-437250138Pas encore d'évaluation
- Catheter Associated Urinary Tract Infections: Running Head: CAUTI Prevention 1Document4 pagesCatheter Associated Urinary Tract Infections: Running Head: CAUTI Prevention 1api-484953296Pas encore d'évaluation
- Catheter-Associated Urinary Tract Infection Care BundleDocument3 pagesCatheter-Associated Urinary Tract Infection Care BundleAnisaPas encore d'évaluation
- Barriers To Urinary Catheter Insertion and Management PracticesDocument5 pagesBarriers To Urinary Catheter Insertion and Management PracticesHelmy HanafiPas encore d'évaluation
- Articulo en InglesDocument8 pagesArticulo en Inglesdante yonathan villegas lozanoPas encore d'évaluation
- Peds PresentationDocument31 pagesPeds Presentationapi-247218432Pas encore d'évaluation
- Zurmehly 2018Document6 pagesZurmehly 2018DavennBacudPas encore d'évaluation
- Nurs 363 Ebp Group Project Final Paper 1Document11 pagesNurs 363 Ebp Group Project Final Paper 1api-269170045Pas encore d'évaluation
- Data Collection ProtocolDocument2 pagesData Collection ProtocolSinung BawonoPas encore d'évaluation
- Final Cauti Leadership Analysis Paper Nurs440Document9 pagesFinal Cauti Leadership Analysis Paper Nurs440api-251662522Pas encore d'évaluation
- A Nurse-Driven Process For TimelyDocument7 pagesA Nurse-Driven Process For TimelyWardah Fauziah El SofwanPas encore d'évaluation
- 440 Leadership Strategic AnalysisDocument7 pages440 Leadership Strategic Analysisapi-212894173Pas encore d'évaluation
- ISID_InfectionGuide_Chapter16Document15 pagesISID_InfectionGuide_Chapter16Nishtha Singh ChauhanPas encore d'évaluation
- PDFDocument9 pagesPDFEven Un Holic100% (1)
- Hospital Quality IndicatorsDocument32 pagesHospital Quality Indicatorsakhtarulmunim2279Pas encore d'évaluation
- Ebp Cauti Research PaperDocument11 pagesEbp Cauti Research Paperapi-598708595Pas encore d'évaluation
- Guideline For Prevention of Catheter-Associated Urinary Tract Infections 2009Document8 pagesGuideline For Prevention of Catheter-Associated Urinary Tract Infections 2009Helmy HanafiPas encore d'évaluation
- ProtocolDocument5 pagesProtocoldrahmedeldaba2Pas encore d'évaluation
- HAI bUNDLESDocument54 pagesHAI bUNDLESNurhayati100% (1)
- Quality Control in Endoscopy Unit: Safety Considerations For The PatientDocument13 pagesQuality Control in Endoscopy Unit: Safety Considerations For The PatientPamela PampamPas encore d'évaluation
- Bundles in Infection Prevention and SafetyDocument15 pagesBundles in Infection Prevention and SafetyInfectologia DiagnosticaPas encore d'évaluation
- Week 6 CisDocument15 pagesWeek 6 Cisapi-302732994Pas encore d'évaluation
- Car SeatDocument3 pagesCar Seatapi-302732994Pas encore d'évaluation
- Wse 4Document4 pagesWse 4api-302732994Pas encore d'évaluation
- Mini Care Plan 4aDocument2 pagesMini Care Plan 4aapi-302732994Pas encore d'évaluation
- Hyperbilirubinemia PathoDocument1 pageHyperbilirubinemia Pathoapi-302732994Pas encore d'évaluation
- Week 4 Reflective JournalDocument2 pagesWeek 4 Reflective Journalapi-302732994Pas encore d'évaluation
- Stages of LaborDocument2 pagesStages of Laborapi-302732994Pas encore d'évaluation
- BreastfeedingDocument2 pagesBreastfeedingapi-302732994Pas encore d'évaluation
- La Leche LeagueDocument5 pagesLa Leche Leagueapi-302732994Pas encore d'évaluation
- Ob PesiDocument3 pagesOb Pesiapi-302732994Pas encore d'évaluation
- FamilyplanninghandoutDocument4 pagesFamilyplanninghandoutapi-302732994Pas encore d'évaluation
- Wse 6Document3 pagesWse 6api-302732994Pas encore d'évaluation
- 2care Plan n360Document1 page2care Plan n360api-302732994Pas encore d'évaluation
- Student Activities On UnitDocument3 pagesStudent Activities On Unitapi-302732994Pas encore d'évaluation
- Eportfolio ResumeDocument2 pagesEportfolio Resumeapi-302732994Pas encore d'évaluation
- 2care Plan 2 n360Document5 pages2care Plan 2 n360api-302732994Pas encore d'évaluation
- Nursing Program'S Student Learning OutcomesDocument1 pageNursing Program'S Student Learning Outcomesapi-302732994Pas encore d'évaluation
- 2capstone 10 10 15Document9 pages2capstone 10 10 15api-302732994Pas encore d'évaluation
- FamilyplanningprojectDocument18 pagesFamilyplanningprojectapi-302732994Pas encore d'évaluation
- n362 Professional Dev PlanDocument4 pagesn362 Professional Dev Planapi-302732994Pas encore d'évaluation
- Process RecordingDocument12 pagesProcess Recordingapi-302732994100% (4)
- Ethical Dilemma Debate - Assisted SuicideDocument23 pagesEthical Dilemma Debate - Assisted SuicidepetitepetalsPas encore d'évaluation
- Ckahepearecommendation 2Document1 pageCkahepearecommendation 2api-302732994Pas encore d'évaluation
- Generic Letter of Reference - Kaua 2Document1 pageGeneric Letter of Reference - Kaua 2api-302732994Pas encore d'évaluation
- Prenatal care case report Philippines municipalityDocument1 pagePrenatal care case report Philippines municipalityMelvin Aurelio100% (1)
- 2014 Present Simple (All Verbs)Document3 pages2014 Present Simple (All Verbs)David Angel Gonzalez ManceraPas encore d'évaluation
- Case StudyDocument9 pagesCase Studyrohan100% (1)
- Smith Peedell (2014) Private Sector and The NHS DebateDocument3 pagesSmith Peedell (2014) Private Sector and The NHS DebateMarinaPapaPas encore d'évaluation
- Dental Radiography & Infection Control QuizDocument12 pagesDental Radiography & Infection Control QuizFaye Nervanna Alecha AlferezPas encore d'évaluation
- SEIU-UHW Executive Board Minutes: June 2016Document1 pageSEIU-UHW Executive Board Minutes: June 2016Anonymous iC9QziKPas encore d'évaluation
- Paediatric Physician Training - FAQ 2017Document4 pagesPaediatric Physician Training - FAQ 2017DrSajid BuzdarPas encore d'évaluation
- Pattern of Dental Caries in Mulago Dental School Clinic, UgandaDocument4 pagesPattern of Dental Caries in Mulago Dental School Clinic, UgandaNeil DolendoPas encore d'évaluation
- 35 Protocol Pharmacologikal Treatment PDFDocument35 pages35 Protocol Pharmacologikal Treatment PDFdragutinpetric100% (1)
- Lung Center VS Quezon CityDocument4 pagesLung Center VS Quezon CityJesstonieCastañaresDamayoPas encore d'évaluation
- Online Job Application for Staff Nurse Position in UAEDocument3 pagesOnline Job Application for Staff Nurse Position in UAEremzyliciousPas encore d'évaluation
- The Investigation of Interferences in Immunoassay: ArticleDocument7 pagesThe Investigation of Interferences in Immunoassay: ArticleAirene ZulfikarPas encore d'évaluation
- Ugly - 1 y 2Document28 pagesUgly - 1 y 2Jesús García LópezPas encore d'évaluation
- Lista e Librave MjekesoreDocument4 pagesLista e Librave MjekesoreEmily OwenPas encore d'évaluation
- Ribbond: A Reinforced Polyethylene Ribbon: - Boon To PedodontistDocument21 pagesRibbond: A Reinforced Polyethylene Ribbon: - Boon To Pedodontistdr parveen bathlaPas encore d'évaluation
- Antimicrobial StewardshipDocument11 pagesAntimicrobial StewardshipMiftahurrahmah GmsPas encore d'évaluation
- Policy of Retention & DestructionDocument6 pagesPolicy of Retention & Destructionumeshbharti0% (1)
- Tongue Cave A TAD Supported Customized Habit Breaking ApplianceDocument3 pagesTongue Cave A TAD Supported Customized Habit Breaking ApplianceInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Management of Sacral Dimples Detected On Routine Newborn Examination: A Case Series and ReviewDocument3 pagesManagement of Sacral Dimples Detected On Routine Newborn Examination: A Case Series and ReviewDesta FransiscaPas encore d'évaluation
- Organisations Working On Donations of Medical Equipment: 1. THET and Partnerships For Global HealthDocument8 pagesOrganisations Working On Donations of Medical Equipment: 1. THET and Partnerships For Global HealthWaynakay RDPas encore d'évaluation
- Medical Reimbursement Check SlipDocument7 pagesMedical Reimbursement Check SlipwasimiitdPas encore d'évaluation
- Legal Aspects of NursingDocument26 pagesLegal Aspects of NursingJasmin Jacob100% (1)
- Case Study (MCN II)Document16 pagesCase Study (MCN II)Gabrielle SandovalPas encore d'évaluation
- Atlas of Procedures in Neonatology PDFDocument446 pagesAtlas of Procedures in Neonatology PDFAndreea Anghelescu100% (1)
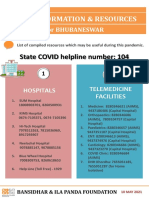
- State COVID Helpline Number: 104Document4 pagesState COVID Helpline Number: 104Yugant NayakPas encore d'évaluation
- Documentation in NursingDocument43 pagesDocumentation in NursingMAHMOOD AHMED100% (19)
- SRS Master Login ModuleDocument17 pagesSRS Master Login ModuleMuneeba KaleemPas encore d'évaluation
- 008 Handbook For Isolation RequrementDocument28 pages008 Handbook For Isolation RequrementAbraham JyothimonPas encore d'évaluation
- Gateway B1 Test Unit 4Document9 pagesGateway B1 Test Unit 4Semir Omerdić75% (20)