Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Apta Lab Values Resource 2013Document3 pagesApta Lab Values Resource 2013api-293223028Pas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Task-Specific TrainingDocument16 pagesTask-Specific Trainingapi-293223028Pas encore d'évaluation
- Yashashree CX LeadsDocument3 pagesYashashree CX LeadsWilfred DsouzaPas encore d'évaluation
- Article - Children Need To Play With Summary AssignmentDocument6 pagesArticle - Children Need To Play With Summary Assignmentjuanjones5Pas encore d'évaluation
- Final Reflection: Social JusticeDocument2 pagesFinal Reflection: Social Justiceapi-293223028Pas encore d'évaluation
- Final Reflection: Evidence-Based Practice (EBP)Document2 pagesFinal Reflection: Evidence-Based Practice (EBP)api-293223028Pas encore d'évaluation
- Occupational Profile and Intervention Plan FinalDocument21 pagesOccupational Profile and Intervention Plan Finalapi-293223028Pas encore d'évaluation
- Assistive Technology PaperDocument12 pagesAssistive Technology Paperapi-293223028Pas encore d'évaluation
- 523 Qualitative PaperDocument16 pages523 Qualitative Paperapi-293223028Pas encore d'évaluation
- Occupational Analysis Intervention PlanDocument19 pagesOccupational Analysis Intervention Planapi-293223028Pas encore d'évaluation
- Occupational ProfileDocument21 pagesOccupational Profileapi-293223028100% (1)
- College Wise Pass PercentageDocument6 pagesCollege Wise Pass PercentageShanawar BasraPas encore d'évaluation
- Community Development: A Critical Approach (Second Edition) : Book ReviewDocument3 pagesCommunity Development: A Critical Approach (Second Edition) : Book ReviewMiko FernandezPas encore d'évaluation
- Family Involvement - How Do I Help My Child Study - ChieSB - FDocument5 pagesFamily Involvement - How Do I Help My Child Study - ChieSB - FChie SBPas encore d'évaluation
- MBA in Healthcare Management - Masters in Hospital AdministrationDocument2 pagesMBA in Healthcare Management - Masters in Hospital AdministrationSandeep SonawnePas encore d'évaluation
- Perdev 2qDocument1 pagePerdev 2qGrace Mary Tedlos BoocPas encore d'évaluation
- Week 7 Lesson Plans 2Document4 pagesWeek 7 Lesson Plans 2api-334646577Pas encore d'évaluation
- Iot Assignment 2Document8 pagesIot Assignment 2Meera SahooPas encore d'évaluation
- Information Brochure & Guidelines For Filling of Online Application Form For Recruitment of Non-Teaching Positions in Delhi UniversityDocument106 pagesInformation Brochure & Guidelines For Filling of Online Application Form For Recruitment of Non-Teaching Positions in Delhi UniversityVidhiLegal BlogPas encore d'évaluation
- Drivers Ed Homework AnswersDocument7 pagesDrivers Ed Homework Answersafnogtyaiergwk100% (1)
- Your Best Chance For: International OffersDocument9 pagesYour Best Chance For: International Offersumesh kumarPas encore d'évaluation
- Collocation SDocument2 pagesCollocation SpatykcPas encore d'évaluation
- The Stage Approach: Developed by W. Huitt (1999)Document39 pagesThe Stage Approach: Developed by W. Huitt (1999)Ruchika AgarwalPas encore d'évaluation
- Fampulme - The Planning Functions of The ControllershipDocument22 pagesFampulme - The Planning Functions of The ControllershipCarla Pianz FampulmePas encore d'évaluation
- NRS110 Lecture 1 Care Plan WorkshopDocument14 pagesNRS110 Lecture 1 Care Plan WorkshopsamehPas encore d'évaluation
- Dual-Attention GAN For Large-Pose Face FrontalizationDocument8 pagesDual-Attention GAN For Large-Pose Face FrontalizationGuillaume Vermeille SanchezPas encore d'évaluation
- 1st QE Grade 11 English 2019-20Document7 pages1st QE Grade 11 English 2019-20Mihatsu TakiPas encore d'évaluation
- Information Technology Project Management - Fifth Edition: by Jack T. Marchewka Northern Illinois UniversityDocument31 pagesInformation Technology Project Management - Fifth Edition: by Jack T. Marchewka Northern Illinois UniversitytofuPas encore d'évaluation
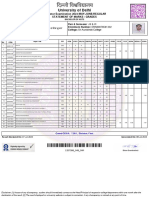
- University of Delhi: Semester Examination 2023-MAY-JUNE:REGULAR Statement of Marks / GradesDocument2 pagesUniversity of Delhi: Semester Examination 2023-MAY-JUNE:REGULAR Statement of Marks / GradesFit CollegePas encore d'évaluation
- Demo K-12 Math Using 4a's Diameter of CircleDocument4 pagesDemo K-12 Math Using 4a's Diameter of CircleMichelle Alejo CortezPas encore d'évaluation
- Nutech University Admission SlipDocument3 pagesNutech University Admission SlipaliiiiPas encore d'évaluation
- Astronauts ScriptDocument3 pagesAstronauts ScriptakkurayhanPas encore d'évaluation
- The Effect of Mindset On Decision-MakingDocument27 pagesThe Effect of Mindset On Decision-MakingJessica PhamPas encore d'évaluation
- Incorporating Music Videos in Theory CoursesDocument5 pagesIncorporating Music Videos in Theory Coursesapi-246372446Pas encore d'évaluation
- Emergence of OBDocument4 pagesEmergence of OBBhavya VermaPas encore d'évaluation
- English Test Unit 1 3rd GradeDocument3 pagesEnglish Test Unit 1 3rd GradeJasmín GálvezPas encore d'évaluation
- Grammar D - Types of Processes in Experiential Meaning (Part 1)Document13 pagesGrammar D - Types of Processes in Experiential Meaning (Part 1)Dena BenPas encore d'évaluation
- Mslearn dp100 14Document2 pagesMslearn dp100 14Emily RapaniPas encore d'évaluation
- B1 Complete PackageDocument69 pagesB1 Complete PackageKhin San ThitPas encore d'évaluation