Vous aimerez peut-être aussi
- Infection Control BrochureDocument2 pagesInfection Control BrochureTeguh Aprian Maulana GultomPas encore d'évaluation
- Phlebotomy LectureDocument195 pagesPhlebotomy Lecturegjob100% (1)
- Infection Control Full GuidelineDocument257 pagesInfection Control Full GuidelinedimkarampPas encore d'évaluation
- Evidence Based PracticeDocument4 pagesEvidence Based PracticeMark EniegoPas encore d'évaluation
- Pneumonia Teaching PlanDocument5 pagesPneumonia Teaching PlanFhai Escio71% (7)
- Lecuniversal PrecautionsDocument34 pagesLecuniversal PrecautionsRabia TahirPas encore d'évaluation
- Lab Safety TrainingDocument105 pagesLab Safety TrainingSabry SaidPas encore d'évaluation
- Bloodborne Training 2018 PDFDocument54 pagesBloodborne Training 2018 PDFIzzuddin FathoniPas encore d'évaluation
- Wing Commander (DR) Suresh Tahiliani AIMA-Accredited Management TeacherDocument50 pagesWing Commander (DR) Suresh Tahiliani AIMA-Accredited Management TeacherMehak KapoorPas encore d'évaluation
- Power Poin Pneumonia, Ispa Dan Diare Maret 2017Document39 pagesPower Poin Pneumonia, Ispa Dan Diare Maret 2017Oscar IhaPas encore d'évaluation
- Hoeltke Chapter2 RevisedDocument44 pagesHoeltke Chapter2 RevisedKarby LeePas encore d'évaluation
- Patient Safety WHO CurriculumDocument46 pagesPatient Safety WHO CurriculumCalvin Chowder WittelsbachPas encore d'évaluation
- Am HCW Safety enDocument2 pagesAm HCW Safety en<_>Pas encore d'évaluation
- Universal Precautions QuizDocument8 pagesUniversal Precautions Quizaakurugu366Pas encore d'évaluation
- IC Clinical StaffDocument41 pagesIC Clinical StaffphysioPas encore d'évaluation
- Practice Standards: Communicable Diseases: Preventing Practitioner-To-Patient TransmissionDocument3 pagesPractice Standards: Communicable Diseases: Preventing Practitioner-To-Patient TransmissionBob100% (1)
- Universal PrecautionsDocument57 pagesUniversal PrecautionsitsdivyanshudcPas encore d'évaluation
- bbp2 Regulations OverviewDocument36 pagesbbp2 Regulations Overviewapi-308826929Pas encore d'évaluation
- Management of Infection Prevention and ControlDocument20 pagesManagement of Infection Prevention and ControlAnna DixonPas encore d'évaluation
- 03.CDC Standard Precautions 22Document22 pages03.CDC Standard Precautions 22Hosam GomaaPas encore d'évaluation
- Universal Precautions Quiz 14 15Document8 pagesUniversal Precautions Quiz 14 15O.r. CadzPas encore d'évaluation
- Bloodborne Pathogens TrainingDocument28 pagesBloodborne Pathogens TrainingPeter GolanskiPas encore d'évaluation
- Infection Control Protocols at Travancore Medical College HospitalDocument8 pagesInfection Control Protocols at Travancore Medical College Hospitaltummalapalli venkateswara raoPas encore d'évaluation
- Is Universal PrecautionsDocument2 pagesIs Universal Precautionsgulamg21Pas encore d'évaluation
- Ethical Issues in HIV Vaccine Trial (Notes)Document63 pagesEthical Issues in HIV Vaccine Trial (Notes)Nuur Mursyiidah MuhammadPas encore d'évaluation
- Module TM1:: 08 Understanding Clinical & Biomedical TerminologyDocument29 pagesModule TM1:: 08 Understanding Clinical & Biomedical TerminologyLarry CalubagPas encore d'évaluation
- Standard Precaution: Prof. Dr. Ida Parwati, PHDDocument23 pagesStandard Precaution: Prof. Dr. Ida Parwati, PHDPutri Senna Rahayu100% (2)
- 0907 UniversalDocument6 pages0907 UniversalRenisa HutahaeanPas encore d'évaluation
- Bloodborne Pathogens: The Occupational Safety and Health Administration StandardDocument55 pagesBloodborne Pathogens: The Occupational Safety and Health Administration StandardfatmawatiPas encore d'évaluation
- Bloodborne PathogensDocument4 pagesBloodborne PathogensMaryNguyenPas encore d'évaluation
- SPECIAL PROCEDURES and INTERDEPENDENT CAREDocument30 pagesSPECIAL PROCEDURES and INTERDEPENDENT CAREcoco brillqntePas encore d'évaluation
- APhA - The Pharmacy Technician, 4th EditionDocument51 pagesAPhA - The Pharmacy Technician, 4th EditionLina TasamaPas encore d'évaluation
- Chapter 5 - Health and SafetyDocument18 pagesChapter 5 - Health and SafetyLalita A/P AnbarasenPas encore d'évaluation
- Universal Precautions Transmission Based PrecautionsDocument61 pagesUniversal Precautions Transmission Based PrecautionsShalamPas encore d'évaluation
- BBP3 ADocument67 pagesBBP3 AMostafa AbdullahPas encore d'évaluation
- Universal Precautions-Judy Smith 211990 7Document19 pagesUniversal Precautions-Judy Smith 211990 7Nurul HusnaPas encore d'évaluation
- Ams Ipc SlidesDocument36 pagesAms Ipc SlidesHarriet TembaPas encore d'évaluation
- Near DrowningDocument15 pagesNear DrowningshenysusantisinaPas encore d'évaluation
- Infection Prevention and Control (IPC) For COVID-19: 3 April 2020Document89 pagesInfection Prevention and Control (IPC) For COVID-19: 3 April 2020Rahmiati LaoPas encore d'évaluation
- Bloodborne Pathogens: Module Nr. 12Document55 pagesBloodborne Pathogens: Module Nr. 12Kh MoPas encore d'évaluation
- Information Package-Nursing Practicum I STUDENTDocument36 pagesInformation Package-Nursing Practicum I STUDENTPui Pui LamPas encore d'évaluation
- Laboratory SafetyDocument30 pagesLaboratory SafetyEliana Nicole IbongPas encore d'évaluation
- Infection Control in Dental Practice 2009Document3 pagesInfection Control in Dental Practice 2009wildernest1Pas encore d'évaluation
- Universal Safety (Health) PrecautionsDocument61 pagesUniversal Safety (Health) Precautionstummalapalli venkateswara rao100% (2)
- DMAC 18 Rev. 1 - December 2010 Human Immunodeficiency Virus (HIV) - Published Nov 27 2012Document2 pagesDMAC 18 Rev. 1 - December 2010 Human Immunodeficiency Virus (HIV) - Published Nov 27 2012C. de JongPas encore d'évaluation
- Universal PrecautionsDocument19 pagesUniversal PrecautionsFatima M67% (3)
- 13 - Bloodborn PathogenDocument55 pages13 - Bloodborn PathogenghufranahmedkhanPas encore d'évaluation
- Module Infectious and InflammatoryDocument6 pagesModule Infectious and InflammatoryMerald PerdigonPas encore d'évaluation
- Needle Sticks Sharps Injuries: FactsDocument31 pagesNeedle Sticks Sharps Injuries: FactsDr. Ashish Jawarkar67% (3)
- 2-ISS - Bloodborne PathogensDocument46 pages2-ISS - Bloodborne PathogensIsmail KamelPas encore d'évaluation
- Health and Hygiene: Level 1Document58 pagesHealth and Hygiene: Level 1RicardoPas encore d'évaluation
- Evidenced Based (Bernardo, BSN - 3C)Document8 pagesEvidenced Based (Bernardo, BSN - 3C)Jerico CunananPas encore d'évaluation
- Hepa B Prevention in The WorkplaceDocument44 pagesHepa B Prevention in The WorkplaceWilliam Alexander Matsuhara AlegrePas encore d'évaluation
- Universal PrecautionDocument39 pagesUniversal PrecautionSyifa MustikaPas encore d'évaluation
- ID EVD SudanVirusUganda EVDOverview 2022-11-02Document43 pagesID EVD SudanVirusUganda EVDOverview 2022-11-02Alan AzadPas encore d'évaluation
- Guidelines For The Management of Occupational Exposures To HBV, HCV, and HIV and Recommendations For Postexposure ProphylaxisDocument58 pagesGuidelines For The Management of Occupational Exposures To HBV, HCV, and HIV and Recommendations For Postexposure ProphylaxisvenkayammaPas encore d'évaluation
- Prophylactic Measures: Sneha Ganesh 2 Yr MbbsDocument25 pagesProphylactic Measures: Sneha Ganesh 2 Yr MbbsSneha GaneshPas encore d'évaluation
- Information ManagementDocument7 pagesInformation ManagementLey EnhaimaPas encore d'évaluation
- Deal Infection ControlDocument98 pagesDeal Infection ControlManuel KituziPas encore d'évaluation
- Nursing care process in patients with chronic obstructive pulmonary diseaseD'EverandNursing care process in patients with chronic obstructive pulmonary diseasePas encore d'évaluation
- Key Terms Chapter 3Document3 pagesKey Terms Chapter 3api-281340024Pas encore d'évaluation
- A P Academic StandardsDocument9 pagesA P Academic Standardsapi-281340024Pas encore d'évaluation
- Chapter 19 Key TermsDocument2 pagesChapter 19 Key Termsapi-281340024Pas encore d'évaluation
- Key Terms Chapter 5 GastrointestinalDocument3 pagesKey Terms Chapter 5 Gastrointestinalapi-281340024Pas encore d'évaluation
- Chapter 4 Key TermsDocument7 pagesChapter 4 Key Termsapi-281340024Pas encore d'évaluation
- Chapter Five Key TermsDocument1 pageChapter Five Key Termsapi-281340024Pas encore d'évaluation
- Med Term Syllabus 2016-2017Document5 pagesMed Term Syllabus 2016-2017api-281340024Pas encore d'évaluation
- National Health Care StandardsDocument9 pagesNational Health Care Standardsapi-281340024Pas encore d'évaluation
- Chapter 2 Key TermsDocument3 pagesChapter 2 Key Termsapi-281340024Pas encore d'évaluation
- Lost at SeaDocument1 pageLost at Seaapi-281340024Pas encore d'évaluation
- Key Terms Chapter 1 Basic Word StructureDocument2 pagesKey Terms Chapter 1 Basic Word Structureapi-281340024Pas encore d'évaluation
- Chapter 10 Key TermsDocument3 pagesChapter 10 Key Termsapi-281340024Pas encore d'évaluation
- Chapter 2 VocabularyDocument1 pageChapter 2 Vocabularyapi-281340024Pas encore d'évaluation
- Health Careers I Syllabus 2016-2017Document5 pagesHealth Careers I Syllabus 2016-2017api-281340024Pas encore d'évaluation
- Practical Review Sheet Foot and ToesDocument2 pagesPractical Review Sheet Foot and Toesapi-281340024Pas encore d'évaluation
- Orthopedic Shoulder ExaminationDocument4 pagesOrthopedic Shoulder Examinationapi-281340024Pas encore d'évaluation
- Health Science Education I Course Description and Academic StandardsDocument5 pagesHealth Science Education I Course Description and Academic Standardsapi-281340024Pas encore d'évaluation
- Blood Chapter 13 Key TermsDocument2 pagesBlood Chapter 13 Key Termsapi-281340024Pas encore d'évaluation
- Key Terms Chapter 14 LymphDocument1 pageKey Terms Chapter 14 Lymphapi-281340024Pas encore d'évaluation
- Key Terms Chapter 15Document3 pagesKey Terms Chapter 15api-281340024Pas encore d'évaluation
- Pren9e PPT CH 14Document37 pagesPren9e PPT CH 14api-281340024Pas encore d'évaluation
- Prentice9e PPT ch13Document39 pagesPrentice9e PPT ch13api-281340024Pas encore d'évaluation
- Chapter 010Document67 pagesChapter 010api-281340024100% (1)
- Thigh Hip and Pelvis ExaminationDocument6 pagesThigh Hip and Pelvis Examinationapi-281340024Pas encore d'évaluation
- Chapter 12 Key TermsDocument3 pagesChapter 12 Key Termsapi-281340024Pas encore d'évaluation
- Crutch Fitting and UsageDocument7 pagesCrutch Fitting and Usageapi-281340024100% (1)
- How To Assess Blood PressureDocument2 pagesHow To Assess Blood Pressureapi-281340024Pas encore d'évaluation
- Chapter 8-cDocument7 pagesChapter 8-capi-281340024Pas encore d'évaluation
- Chapter 8-EDocument9 pagesChapter 8-Eapi-281340024Pas encore d'évaluation
- Chapter 8-dDocument10 pagesChapter 8-dapi-281340024Pas encore d'évaluation
- Club 25Document12 pagesClub 25Mithun HaridasPas encore d'évaluation
- OpisthorchisDocument17 pagesOpisthorchisIqraAzizPas encore d'évaluation
- Cold ChainDocument15 pagesCold ChainLok KannPas encore d'évaluation
- Recommended Vaccinations For AdultsDocument1 pageRecommended Vaccinations For AdultsThe Press-Enterprise / pressenterprise.comPas encore d'évaluation
- Management of Patient With AnemiaDocument58 pagesManagement of Patient With AnemiaDoaa HussainPas encore d'évaluation
- Shunt TechnologiesDocument106 pagesShunt TechnologiesalvarogerardmdPas encore d'évaluation
- Albendazol PDFDocument8 pagesAlbendazol PDFDANIBATAPas encore d'évaluation
- Demyelinasi & Peny KongenitalDocument42 pagesDemyelinasi & Peny KongenitalamiraPas encore d'évaluation
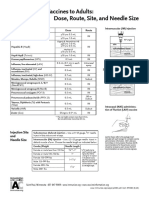
- Administering Vaccines To Adults: Dose, Route, Site, and Needle SizeDocument1 pageAdministering Vaccines To Adults: Dose, Route, Site, and Needle SizeAkashPas encore d'évaluation
- Antibiotic Guidelines (2020) - 0Document55 pagesAntibiotic Guidelines (2020) - 0yudhit bessiePas encore d'évaluation
- Excreta DisposalDocument12 pagesExcreta DisposalfelamendoPas encore d'évaluation
- Blueberry Propagation SuggestionsDocument8 pagesBlueberry Propagation SuggestionsJovan Ličanin100% (1)
- National Guidelines For HIV Testing - 21apr2016Document120 pagesNational Guidelines For HIV Testing - 21apr2016prastacharPas encore d'évaluation
- Bulb Mite Found in Garlic FieldsDocument2 pagesBulb Mite Found in Garlic FieldsRuni Ayu PPas encore d'évaluation
- Cytogen ReviewerDocument4 pagesCytogen ReviewerSophia Mae ClavecillaPas encore d'évaluation
- Pemantauan Bayi Prematur (DR Mei Neni) Nov2015Document33 pagesPemantauan Bayi Prematur (DR Mei Neni) Nov2015nur_beta100% (1)
- Case Study 4 RevisedDocument9 pagesCase Study 4 RevisedHearts heavy Moms spaghettiPas encore d'évaluation
- Integrated Disease Management in Vegetable CropsDocument56 pagesIntegrated Disease Management in Vegetable CropsSavita Bhoutekar100% (1)
- Multisystem & Genetic - BoardsDocument10 pagesMultisystem & Genetic - BoardsSoojung NamPas encore d'évaluation
- Lesi Multipel Akut (Infeksi Virus & Bakteri)Document19 pagesLesi Multipel Akut (Infeksi Virus & Bakteri)Icha AnviniPas encore d'évaluation
- Crimean-Congo Hemorrhagic Fever History, Epidemiology, Pathogenesis, Clinical Syndrome and Genetic DiversityDocument31 pagesCrimean-Congo Hemorrhagic Fever History, Epidemiology, Pathogenesis, Clinical Syndrome and Genetic DiversityfaizalPas encore d'évaluation
- 2006 Surgery Final 6th YearDocument13 pages2006 Surgery Final 6th Yearmarina_shawkyPas encore d'évaluation
- Genital Tract InfectionDocument48 pagesGenital Tract InfectionMohanBabuPas encore d'évaluation
- Final Research Paper 1 Enc 1102 Tamryn Webb-GurleyDocument11 pagesFinal Research Paper 1 Enc 1102 Tamryn Webb-Gurleyapi-490436143100% (1)
- Pathology Lecture SeriesDocument168 pagesPathology Lecture SeriesButch DumdumPas encore d'évaluation
- Bacte Notes #1 - Introduction To BacteriologyDocument14 pagesBacte Notes #1 - Introduction To BacteriologyMartin ClydePas encore d'évaluation
- RabiesDocument32 pagesRabiesKareen Mae Porras BienePas encore d'évaluation
- Fracture Repair and Bone GraftingDocument10 pagesFracture Repair and Bone GraftingaiakobyPas encore d'évaluation
- Role of Viral Infection in Sudden Hearing Loss: Xin Chen, Yao-Yao Fu and Tian-Yu ZhangDocument8 pagesRole of Viral Infection in Sudden Hearing Loss: Xin Chen, Yao-Yao Fu and Tian-Yu Zhanggeraldi radityaPas encore d'évaluation