Vous aimerez peut-être aussi
- Maternal-Newborn Nursing DeMYSTiFieD: A Self-Teaching GuideD'EverandMaternal-Newborn Nursing DeMYSTiFieD: A Self-Teaching GuidePas encore d'évaluation
- Notes-Maternal Health NursingDocument22 pagesNotes-Maternal Health NursingRachael Crossgrove100% (4)
- Schaum's Outline of Maternal-Newborn Nursing: 700 Review QuestionsD'EverandSchaum's Outline of Maternal-Newborn Nursing: 700 Review QuestionsPas encore d'évaluation
- Maternal NursingDocument37 pagesMaternal NursingCai Velasco DecenaPas encore d'évaluation
- MATERNAL AND CHILD HEALTH NURSE: Passbooks Study GuideD'EverandMATERNAL AND CHILD HEALTH NURSE: Passbooks Study GuidePas encore d'évaluation
- Maternity NursingDocument10 pagesMaternity NursingJustine Jake L. Ella100% (7)
- 2020 NCLEX-PN Test Prep. Questions and Answers with Explanations: Study Guide to Pass the License Exam Effortlessly - Exam Review for Practical NursesD'Everand2020 NCLEX-PN Test Prep. Questions and Answers with Explanations: Study Guide to Pass the License Exam Effortlessly - Exam Review for Practical NursesÉvaluation : 1 sur 5 étoiles1/5 (1)
- Obstetric Nursing Review (NLE)Document48 pagesObstetric Nursing Review (NLE)'jmark Francia100% (4)
- Inpatient Obstetric Nurse Exam Prep 2020-2021: A New Study Guide for Certification Including 300 Test Questions and Answers with Full Explanations (RNC-OB)D'EverandInpatient Obstetric Nurse Exam Prep 2020-2021: A New Study Guide for Certification Including 300 Test Questions and Answers with Full Explanations (RNC-OB)Pas encore d'évaluation
- Maternal & Child Care Nursing ReviewDocument37 pagesMaternal & Child Care Nursing Reviewɹǝʍdןnos98% (130)
- FUNDAMENTALS OF NURSING: Passbooks Study GuideD'EverandFUNDAMENTALS OF NURSING: Passbooks Study GuideÉvaluation : 5 sur 5 étoiles5/5 (1)
- Maternal and Child Health Nursing ReviewerDocument17 pagesMaternal and Child Health Nursing ReviewerJeffrey Viernes100% (6)
- 1 - Maternal and Child Health Nursing PracticeDocument57 pages1 - Maternal and Child Health Nursing PracticePatricia Anne Nicole Cuaresma100% (4)
- COMMUNITY HEALTH NURSE: Passbooks Study GuideD'EverandCOMMUNITY HEALTH NURSE: Passbooks Study GuidePas encore d'évaluation
- Pediatric NursingDocument55 pagesPediatric Nursingbajaoc100% (14)
- MEDICAL SURGICAL NURSING: Passbooks Study GuideD'EverandMEDICAL SURGICAL NURSING: Passbooks Study GuidePas encore d'évaluation
- Pediatric Nursing PDFDocument15 pagesPediatric Nursing PDFAte Icé100% (4)
- Maternity NursingDocument40 pagesMaternity NursingClarissa Guifaya100% (2)
- Maternity Nursing ReviewDocument54 pagesMaternity Nursing ReviewJr Robis100% (6)
- Chicago Review Press NCLEX-PN Practice Test and ReviewD'EverandChicago Review Press NCLEX-PN Practice Test and ReviewÉvaluation : 4 sur 5 étoiles4/5 (4)
- Maternal & Newborn Nursing ExamDocument3 pagesMaternal & Newborn Nursing ExamPaul Jhon Vergara88% (25)
- 2017 NCLEX-RN Test Prep Questions and Answers with Explanations: Study Guide to Pass the License Exam EffortlesslyD'Everand2017 NCLEX-RN Test Prep Questions and Answers with Explanations: Study Guide to Pass the License Exam EffortlesslyÉvaluation : 4 sur 5 étoiles4/5 (18)
- Obstetrics-Maternal and Child Health Nursing Practice TestDocument13 pagesObstetrics-Maternal and Child Health Nursing Practice TestKira94% (71)
- Lecture Maternal and Child Health NursingDocument6 pagesLecture Maternal and Child Health NursingAmpie EmPas encore d'évaluation
- PEDIATRIC NURSING Review (NLE)Document56 pagesPEDIATRIC NURSING Review (NLE)'jmark Francia100% (4)
- The Everything New Nurse Book: Gain Confidence, Manage your Schedule, and Deal with the UnexpectedD'EverandThe Everything New Nurse Book: Gain Confidence, Manage your Schedule, and Deal with the UnexpectedÉvaluation : 5 sur 5 étoiles5/5 (1)
- Maternity Study GuideDocument43 pagesMaternity Study Guidepgmanski100% (23)
- Nursing HESI A2: a QuickStudy Laminated Reference & Study GuideD'EverandNursing HESI A2: a QuickStudy Laminated Reference & Study GuideÉvaluation : 4 sur 5 étoiles4/5 (1)
- Maternity Nursing Edited Royal PentagonDocument49 pagesMaternity Nursing Edited Royal PentagonRichard Ines Valino95% (38)
- Maternal ExamDocument52 pagesMaternal ExamEdRobertArnad100% (14)
- NCM 101 FinalsDocument3 pagesNCM 101 FinalsPaul Jhon Vergara100% (2)
- Fluid and Electrolytes for Nursing StudentsD'EverandFluid and Electrolytes for Nursing StudentsÉvaluation : 5 sur 5 étoiles5/5 (12)
- Obstetrical Nursing NotesDocument25 pagesObstetrical Nursing NotesFreeNursingNotes81% (16)
- The Basics: A Comprehensive Outline of Nursing School ContentD'EverandThe Basics: A Comprehensive Outline of Nursing School ContentÉvaluation : 5 sur 5 étoiles5/5 (3)
- OB Nursing Test QuestionsDocument15 pagesOB Nursing Test QuestionsAileen Orjaliza Babanto100% (5)
- Gapuz Maternal Health NursingDocument80 pagesGapuz Maternal Health NursingHayes Clover100% (6)
- Maternal and Child Health Nursing ReviewerDocument119 pagesMaternal and Child Health Nursing Reviewerasdf100% (1)
- A Simplified Guide to Nursing Mnemonics (2022 Edition)D'EverandA Simplified Guide to Nursing Mnemonics (2022 Edition)Pas encore d'évaluation
- Fundamentals of NursingDocument29 pagesFundamentals of Nursingblazegomez92% (26)
- Dimensional Analysis For Nursing StudentsD'EverandDimensional Analysis For Nursing StudentsPas encore d'évaluation
- Nursing Notes Maternal and Child Nursing CareDocument70 pagesNursing Notes Maternal and Child Nursing CareAsniah Hadjiadatu AbdullahPas encore d'évaluation
- Gapuz Fundamentals of NursingDocument61 pagesGapuz Fundamentals of Nursingkarendelarosa06277100% (24)
- Schaum's Outline of Emergency Nursing: 242 Review QuestionsD'EverandSchaum's Outline of Emergency Nursing: 242 Review QuestionsÉvaluation : 4.5 sur 5 étoiles4.5/5 (3)
- Maternal & Child NursingDocument15 pagesMaternal & Child NursingLilian Flores100% (2)
- 2018 NCLEX-PN Test Prep. Questions and Answers with Explanations: Study Guide to Pass the License Exam Effortlessly - Exam Review for Practical NursesD'Everand2018 NCLEX-PN Test Prep. Questions and Answers with Explanations: Study Guide to Pass the License Exam Effortlessly - Exam Review for Practical NursesÉvaluation : 4.5 sur 5 étoiles4.5/5 (2)
- Practice Test Maternity-Nsg 100 ItemsDocument21 pagesPractice Test Maternity-Nsg 100 ItemsPaul Christian P. Santos, RN100% (21)
- Maternal & Child Nursing Bullets (Nle & Nclex)Document38 pagesMaternal & Child Nursing Bullets (Nle & Nclex)Richard Ines Valino95% (22)
- NCLEX-PN Prep Plus: 2 Practice Tests + Proven Strategies + Online + VideoD'EverandNCLEX-PN Prep Plus: 2 Practice Tests + Proven Strategies + Online + VideoPas encore d'évaluation
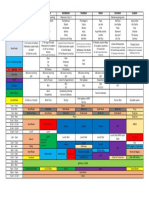
- Monday Tuesday Wednesday Thursday Friday Saturday SundayDocument1 pageMonday Tuesday Wednesday Thursday Friday Saturday SundayWarrenSandovalPas encore d'évaluation
- AsepsisDocument7 pagesAsepsisWarrenSandovalPas encore d'évaluation
- OB Definition of TermsDocument9 pagesOB Definition of TermsWarrenSandovalPas encore d'évaluation
- Principles and Elements of Floral DesignDocument104 pagesPrinciples and Elements of Floral DesignWarrenSandoval100% (2)
- DiaphragmsDocument16 pagesDiaphragmsWarrenSandovalPas encore d'évaluation
- First Aid KitDocument65 pagesFirst Aid KitWarrenSandovalPas encore d'évaluation
- Principles of CaregivingDocument196 pagesPrinciples of CaregivingWarrenSandoval100% (4)
- Radical Love in F#MDocument2 pagesRadical Love in F#MWarrenSandovalPas encore d'évaluation
- The King (For Sharing)Document5 pagesThe King (For Sharing)WarrenSandovalPas encore d'évaluation
- Victorious God (1 of 2) : KeyofbDocument2 pagesVictorious God (1 of 2) : KeyofbWarrenSandovalPas encore d'évaluation
- The King (For Sharing)Document5 pagesThe King (For Sharing)WarrenSandovalPas encore d'évaluation
- HormoneDocument5 pagesHormoneWarrenSandovalPas encore d'évaluation
- HY-TB3DV-M 3axis Driver PDFDocument10 pagesHY-TB3DV-M 3axis Driver PDFjoelgcrPas encore d'évaluation
- Contact Inform 2002 PDFDocument24 pagesContact Inform 2002 PDFFrank AlmeidaPas encore d'évaluation
- DS Ltch00601daa0 R05Document4 pagesDS Ltch00601daa0 R05rajareddy235Pas encore d'évaluation
- DEEP ECOLOGY - An Intro - McLaughlinDocument5 pagesDEEP ECOLOGY - An Intro - McLaughlinCarlo MagcamitPas encore d'évaluation
- Science Involved in Floating Paper Clip Science Experiment GuidelinesDocument4 pagesScience Involved in Floating Paper Clip Science Experiment GuidelinesSHIELA RUBIOPas encore d'évaluation
- 10th Aug. 2011 Structural Calculation (For Sub.) - 03Document29 pages10th Aug. 2011 Structural Calculation (For Sub.) - 03Nguyễn Tiến Việt100% (1)
- Binder 3 of 4 Dec-2018Document1 169 pagesBinder 3 of 4 Dec-2018Anonymous OEmUQuPas encore d'évaluation
- Propert 447-445Document11 pagesPropert 447-445LUNA100% (1)
- Mathematical Modeling of Mechanical Systems and Electrical SystemsDocument49 pagesMathematical Modeling of Mechanical Systems and Electrical SystemsMary DunhamPas encore d'évaluation
- 1986 EMT Disruption of Microbial Cells For Intracellular ProductsDocument11 pages1986 EMT Disruption of Microbial Cells For Intracellular ProductsLezid CortesPas encore d'évaluation
- Kuiz1 210114Document12 pagesKuiz1 210114Vincent HoPas encore d'évaluation
- Do Roman Catholics KnOw About The Great Pyramids of China?Document11 pagesDo Roman Catholics KnOw About The Great Pyramids of China?.Pas encore d'évaluation
- Pre RmoDocument4 pagesPre RmoSangeeta Mishra100% (1)
- Imbinari Teava Fibra de Sticla PDFDocument1 pageImbinari Teava Fibra de Sticla PDFplex015Pas encore d'évaluation
- Ecotopia Remixed II-FormattedDocument54 pagesEcotopia Remixed II-FormattedthisisdarrenPas encore d'évaluation
- Convection Concentric Annulus Vertical Cylinders Filling Porous MediaDocument17 pagesConvection Concentric Annulus Vertical Cylinders Filling Porous MediakarthikeyanPas encore d'évaluation
- Active Faults in MalaysiaDocument52 pagesActive Faults in MalaysiaHazim HaPas encore d'évaluation
- SP 73Document105 pagesSP 73Rodrigo Vilanova100% (3)
- ASCE Snow Loads On Solar-Paneled RoofsDocument61 pagesASCE Snow Loads On Solar-Paneled RoofsBen100% (1)
- Stanley B. Alpern - Amazons of Black Sparta - The Women Warriors of Dahomey-New York University Press (2011)Document308 pagesStanley B. Alpern - Amazons of Black Sparta - The Women Warriors of Dahomey-New York University Press (2011)georgemultiplusPas encore d'évaluation
- Complete Processing Lines For Extruded Pet FoodDocument13 pagesComplete Processing Lines For Extruded Pet FoodденисPas encore d'évaluation
- Conformational Analysis: Carey & Sundberg: Part A Chapter 3Document53 pagesConformational Analysis: Carey & Sundberg: Part A Chapter 3Dr-Dinesh Kumar100% (1)
- L2 Biostatistics ProbabilityDocument84 pagesL2 Biostatistics ProbabilityAaron CiudadPas encore d'évaluation
- Monkeys PawDocument4 pagesMonkeys PawKaitlin HartmanPas encore d'évaluation
- 9701 w09 QP 21Document12 pages9701 w09 QP 21Hubbak KhanPas encore d'évaluation
- Brief Summary of Catalytic ConverterDocument23 pagesBrief Summary of Catalytic ConverterjoelPas encore d'évaluation
- How To Eat WellDocument68 pagesHow To Eat WelleledidiPas encore d'évaluation
- SAT Biochar Ethylene Poster 10 - 10b PDFDocument1 pageSAT Biochar Ethylene Poster 10 - 10b PDFsherifalharamPas encore d'évaluation
- Genie GS-1930 Parts ManualDocument194 pagesGenie GS-1930 Parts ManualNestor Matos GarcíaPas encore d'évaluation
- Unit 2 - Presentations (Image, Impact and Making An Impression) 2Document25 pagesUnit 2 - Presentations (Image, Impact and Making An Impression) 2LK Chiarra Panaligan100% (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossD'EverandThe Obesity Code: Unlocking the Secrets of Weight LossÉvaluation : 4 sur 5 étoiles4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDD'EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDÉvaluation : 5 sur 5 étoiles5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeD'EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeÉvaluation : 2 sur 5 étoiles2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (25)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionD'EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionÉvaluation : 4 sur 5 étoiles4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisD'EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisÉvaluation : 4.5 sur 5 étoiles4.5/5 (42)
- The Comfort of Crows: A Backyard YearD'EverandThe Comfort of Crows: A Backyard YearÉvaluation : 4.5 sur 5 étoiles4.5/5 (23)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsD'EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsÉvaluation : 5 sur 5 étoiles5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaD'EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisD'EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsD'EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsPas encore d'évaluation
- Why We Die: The New Science of Aging and the Quest for ImmortalityD'EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityÉvaluation : 4 sur 5 étoiles4/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryD'EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryÉvaluation : 4 sur 5 étoiles4/5 (44)