Vous aimerez peut-être aussi
- Executive SummaryDocument2 pagesExecutive Summaryapi-260169062Pas encore d'évaluation
- Final Data Transformation Presentation-1Document7 pagesFinal Data Transformation Presentation-1api-260169062Pas encore d'évaluation
- Clinical Hour Tracking Spring 2016 Erin BisconeDocument21 pagesClinical Hour Tracking Spring 2016 Erin Bisconeapi-260169062Pas encore d'évaluation
- Clinical Hour Tracking Spring 2016 Erin BisconeDocument21 pagesClinical Hour Tracking Spring 2016 Erin Bisconeapi-260169062Pas encore d'évaluation
- Health Sys Evidence Week 11Document15 pagesHealth Sys Evidence Week 11api-260169062Pas encore d'évaluation
- Acog Distrrict Xi and CTCNM PolicyDocument4 pagesAcog Distrrict Xi and CTCNM Policyapi-260169062Pas encore d'évaluation
- DNP Project Protocol For Texas Dshs Irb ReviewDocument23 pagesDNP Project Protocol For Texas Dshs Irb Reviewapi-260169062Pas encore d'évaluation
- Clinical Hour Tracking Sheet Fall 2015 Erin BisconeDocument24 pagesClinical Hour Tracking Sheet Fall 2015 Erin Bisconeapi-260169062Pas encore d'évaluation
- Clinical Hour Tracking Sheet Summer 2015 Erin BisconeDocument24 pagesClinical Hour Tracking Sheet Summer 2015 Erin Bisconeapi-260169062Pas encore d'évaluation
- Informatics Week 6 Personal Health Record PresentationDocument14 pagesInformatics Week 6 Personal Health Record Presentationapi-260169062Pas encore d'évaluation
- DNP Project Protocol For Texas Dshs Irb ReviewDocument23 pagesDNP Project Protocol For Texas Dshs Irb Reviewapi-260169062Pas encore d'évaluation
- Finance Anthem Paper 2Document14 pagesFinance Anthem Paper 2api-260169062Pas encore d'évaluation
- Health Policy Sterilization PaperDocument6 pagesHealth Policy Sterilization Paperapi-260169062Pas encore d'évaluation
- Informatics N 2 Transforming Maternity CareDocument9 pagesInformatics N 2 Transforming Maternity Careapi-260169062Pas encore d'évaluation
- FinaldatatransformationDocument45 pagesFinaldatatransformationapi-260169062Pas encore d'évaluation
- Lead Complex Week 2Document1 pageLead Complex Week 2api-260169062Pas encore d'évaluation
- Health Econ CbaDocument9 pagesHealth Econ Cbaapi-260169062Pas encore d'évaluation
- Analytics Causal Theory Paper DNP ProjectDocument14 pagesAnalytics Causal Theory Paper DNP Projectapi-260169062Pas encore d'évaluation
- DNP Project 2 Week OneDocument1 pageDNP Project 2 Week Oneapi-260169062Pas encore d'évaluation
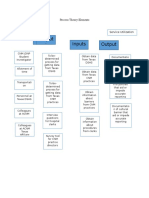
- Analytics - Process Theory ElementsDocument1 pageAnalytics - Process Theory Elementsapi-260169062Pas encore d'évaluation
- Lead Complex Week 5Document2 pagesLead Complex Week 5api-260169062Pas encore d'évaluation
- DNP Semester Sat Presentation Oct 4Document8 pagesDNP Semester Sat Presentation Oct 4api-260169062Pas encore d'évaluation
- Semester Sat Nov 22 Presentation1Document8 pagesSemester Sat Nov 22 Presentation1api-260169062Pas encore d'évaluation
- Oct Writing Workshop Essay On LeadershipDocument6 pagesOct Writing Workshop Essay On Leadershipapi-260169062Pas encore d'évaluation
- Erin Biscone Resume Jan 2016Document2 pagesErin Biscone Resume Jan 2016api-260169062Pas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hitachi Loader Lx70 Lx80 Service Manual KM 111 00yyy FTT HDocument22 pagesHitachi Loader Lx70 Lx80 Service Manual KM 111 00yyy FTT Hmarymurphy140886wdi100% (103)
- Bhavartha Ratnakara: ReferencesDocument2 pagesBhavartha Ratnakara: ReferencescrppypolPas encore d'évaluation
- Electrostatics Formulas and Numerical ProblemsDocument11 pagesElectrostatics Formulas and Numerical ProblemsManish kumar100% (2)
- Ardipithecus Ramidus Is A Hominin Species Dating To Between 4.5 and 4.2 Million Years AgoDocument5 pagesArdipithecus Ramidus Is A Hominin Species Dating To Between 4.5 and 4.2 Million Years AgoBianca IrimiePas encore d'évaluation
- Community Action and Core Values and Principles of Community-Action InitiativesDocument5 pagesCommunity Action and Core Values and Principles of Community-Action Initiativeskimberson alacyangPas encore d'évaluation
- Jason A Brown: 1374 Cabin Creek Drive, Nicholson, GA 30565Document3 pagesJason A Brown: 1374 Cabin Creek Drive, Nicholson, GA 30565Jason BrownPas encore d'évaluation
- Family Health Nursing Process Part 2Document23 pagesFamily Health Nursing Process Part 2Fatima Ysabelle Marie RuizPas encore d'évaluation
- Score:: A. Double - Napped Circular ConeDocument3 pagesScore:: A. Double - Napped Circular ConeCarmilleah FreyjahPas encore d'évaluation
- Leibniz Integral Rule - WikipediaDocument70 pagesLeibniz Integral Rule - WikipediaMannu Bhattacharya100% (1)
- 14 - Habeas Corpus PetitionDocument4 pages14 - Habeas Corpus PetitionJalaj AgarwalPas encore d'évaluation
- Exodus Post Apocalyptic PDF 10Document2 pagesExodus Post Apocalyptic PDF 10RushabhPas encore d'évaluation
- Unit 3 Activity 1-1597187907Document3 pagesUnit 3 Activity 1-1597187907Bryan SaltosPas encore d'évaluation
- Unit 4 Trade Discounts Cash Discounts MarkupDocument42 pagesUnit 4 Trade Discounts Cash Discounts MarkupChimwemwe MaolePas encore d'évaluation
- Thelen Reid Brown Raysman & Steiner LLP - Document No. 7Document1 pageThelen Reid Brown Raysman & Steiner LLP - Document No. 7Justia.comPas encore d'évaluation
- The ADDIE Instructional Design ModelDocument2 pagesThe ADDIE Instructional Design ModelChristopher Pappas100% (1)
- Veerabhadra Swamy MantrasDocument6 pagesVeerabhadra Swamy Mantrasगणेश पराजुलीPas encore d'évaluation
- Great Mobile Application Requirement Document: 7 Steps To Write ADocument11 pagesGreat Mobile Application Requirement Document: 7 Steps To Write AgpchariPas encore d'évaluation
- BtuDocument39 pagesBtuMel Vin100% (1)
- Case DurexDocument3 pagesCase DurexGia ChuongPas encore d'évaluation
- SAP HANA Analytics Training at MAJUDocument1 pageSAP HANA Analytics Training at MAJUXIPas encore d'évaluation
- Dryer User ManualDocument118 pagesDryer User ManualAyman Alhassny100% (1)
- Completing-Your-Copy-With-Captions-And-Headlines Lesson-1Document24 pagesCompleting-Your-Copy-With-Captions-And-Headlines Lesson-1api-294176103Pas encore d'évaluation
- Daily Lesson Plan: Week DAY Date Class Time SubjectDocument3 pagesDaily Lesson Plan: Week DAY Date Class Time SubjectHasanah HassanPas encore d'évaluation
- Bunga Refira - 1830104008 - Allophonic RulesDocument6 pagesBunga Refira - 1830104008 - Allophonic RulesBunga RefiraPas encore d'évaluation
- Social Media Marketing - AssignmentDocument8 pagesSocial Media Marketing - AssignmentAllen RodaPas encore d'évaluation
- FortiMail Log Message Reference v300Document92 pagesFortiMail Log Message Reference v300Ronald Vega VilchezPas encore d'évaluation
- Journal EntriesDocument10 pagesJournal Entriesapi-283322366Pas encore d'évaluation
- Unit 11 LeadershipDocument4 pagesUnit 11 LeadershipMarijana DragašPas encore d'évaluation
- Awareness Training On Filipino Sign Language (FSL) PDFDocument3 pagesAwareness Training On Filipino Sign Language (FSL) PDFEmerito PerezPas encore d'évaluation
- ML Performance Improvement CheatsheetDocument11 pagesML Performance Improvement Cheatsheetrahulsukhija100% (1)