Vous aimerez peut-être aussi
- Nursing Care PlanDocument1 pageNursing Care PlanSHeenah Qo100% (1)
- Benign Prostatic Hyperplasia NCPDocument2 pagesBenign Prostatic Hyperplasia NCPCyrus De Asis100% (2)
- NCP BPHDocument8 pagesNCP BPHjyaba0% (1)
- NCP PancreatitisDocument2 pagesNCP PancreatitisJeanelle Generoso100% (1)
- Urinary Retention, RevisedDocument2 pagesUrinary Retention, RevisedKim Beverly100% (5)
- NCP For Pain - NephrolithiasisDocument3 pagesNCP For Pain - NephrolithiasisDepia Leah NgislawanPas encore d'évaluation
- Liver NCPDocument5 pagesLiver NCPMerrill HansPas encore d'évaluation
- Nursing Care PlansDocument4 pagesNursing Care PlansanreilegardePas encore d'évaluation
- NCPDocument1 pageNCPhaniehaehae100% (1)
- NCP For Urinary RetentionDocument5 pagesNCP For Urinary RetentionColeen Comelle Huerto60% (5)
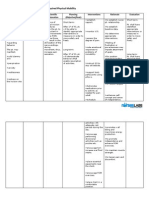
- NURSING CARE PLAN Problem Body Weakness Nursing Diagnosis Impaired PhysicalDocument1 pageNURSING CARE PLAN Problem Body Weakness Nursing Diagnosis Impaired Physicalmitchie riveraPas encore d'évaluation
- Nursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument3 pagesNursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationAbdallah AlasalPas encore d'évaluation
- Impaired Urinary EliminationDocument2 pagesImpaired Urinary EliminationHaon Anasu67% (3)
- Assessment Nursing Diagnosis Planning Implementation Scientific Rationale EvaluationDocument5 pagesAssessment Nursing Diagnosis Planning Implementation Scientific Rationale Evaluationjennelyn losanta100% (2)
- Anatomy and Physiology of Peptic UlcerDocument16 pagesAnatomy and Physiology of Peptic UlcerDrNarayan KR100% (8)
- NCP 2Document2 pagesNCP 2Neil Abraham Mendoza Lalap100% (2)
- Impaired Urinary EliminationDocument3 pagesImpaired Urinary Eliminationcamziii89% (18)
- Preoperative and Post Liver Transplant Nursing Care PlanDocument5 pagesPreoperative and Post Liver Transplant Nursing Care PlanOctoober67% (6)
- Betty Impaired Skin IntegrityDocument2 pagesBetty Impaired Skin IntegrityBenjie DimayacyacPas encore d'évaluation
- Assessment Diagnosis Planning Implementation Evaluation No Subjective Cues ObjectiveDocument3 pagesAssessment Diagnosis Planning Implementation Evaluation No Subjective Cues ObjectiveMaverick LimPas encore d'évaluation
- NCP Risk Infection Papillary Thyroid CADocument2 pagesNCP Risk Infection Papillary Thyroid CAjazvPas encore d'évaluation
- Chiari - Frommel Syndrome - Sexual Dysfunction, Sexual Intercourse Discomfort & Loss of Sexual Desire Related To Dryness in The Vagina Secondary To Gal Actor RheaDocument3 pagesChiari - Frommel Syndrome - Sexual Dysfunction, Sexual Intercourse Discomfort & Loss of Sexual Desire Related To Dryness in The Vagina Secondary To Gal Actor RheaLoord Vie Lu MondigoPas encore d'évaluation
- Nursing Care Plan: Risk For Ineffective Airway Clearance Related To Bleeding From Tonsillectomy Short TermDocument4 pagesNursing Care Plan: Risk For Ineffective Airway Clearance Related To Bleeding From Tonsillectomy Short TermErika Danalle ArceoPas encore d'évaluation
- Iii. Nursing Care PlansDocument13 pagesIii. Nursing Care PlansLharra Cagulada-Postrano100% (1)
- Ovarian Cancer NCPDocument7 pagesOvarian Cancer NCPAsterlyn Coniendo100% (1)
- NCP-impaired Urinary Elimination-TAHBSODocument3 pagesNCP-impaired Urinary Elimination-TAHBSOtinatin9890% (1)
- NCP of Renal CalculiDocument3 pagesNCP of Renal Calculidextroid1289% (9)
- Nursing DiagnosisvfsdsDocument2 pagesNursing DiagnosisvfsdsPrincess Gutierrez Rosita100% (1)
- NCP Visual SensoryDocument2 pagesNCP Visual SensoryEugene UCPas encore d'évaluation
- Case: Liver Cirrhosis Assessment:: Nursing InferenceDocument7 pagesCase: Liver Cirrhosis Assessment:: Nursing InferenceLovelyn GanirPas encore d'évaluation
- Nursing Care Plan NephritisDocument2 pagesNursing Care Plan Nephritisderic82% (17)
- Nursing Care Plan CYSTITISDocument2 pagesNursing Care Plan CYSTITIS@ngelo0% (1)
- Prostate Cancer NCPDocument1 pageProstate Cancer NCPKathleen Dimacali0% (1)
- NCP Liver CirrhosisDocument7 pagesNCP Liver CirrhosisIris Jimenez-BuanPas encore d'évaluation
- NCPDocument8 pagesNCPJoseph Anthony Benitez VerzosaPas encore d'évaluation
- NCP Pancreatic MassDocument4 pagesNCP Pancreatic MassAnonymous XvwKtnSrMR78% (9)
- NCP TesticularDocument8 pagesNCP TesticularPrincess Gutierrez Rosita50% (2)
- Nursing Care Plan: Priority No. 3Document2 pagesNursing Care Plan: Priority No. 3Pantaleon PacisPas encore d'évaluation
- Nursing Care Plan ConstipationDocument2 pagesNursing Care Plan ConstipationGio Baduria100% (1)
- Appendectomy Nursing Care Plan - Risk For InfectionDocument2 pagesAppendectomy Nursing Care Plan - Risk For InfectionChebz Zy0% (1)
- NCP Heart BlockDocument3 pagesNCP Heart BlockEköw Santiago Javier33% (3)
- Activity Intolerance Related To AmeniaDocument1 pageActivity Intolerance Related To AmeniaSiti Syazana Mohamad MogriPas encore d'évaluation
- BPH NCPDocument1 pageBPH NCPJayson BenitezPas encore d'évaluation
- NCP Cellulitis Risk For InfectionDocument3 pagesNCP Cellulitis Risk For Infectionchin ramos50% (2)
- Impaired Physical Mobility CholecystectomyDocument2 pagesImpaired Physical Mobility CholecystectomyPrincess Danica Purcia100% (1)
- NCP Cholecystectomy RevisedDocument7 pagesNCP Cholecystectomy RevisedMariquita Buenafe100% (4)
- Nursing Care PlansDocument48 pagesNursing Care PlansJuliantiMamangkey86% (7)
- Impaired Gas Exchange Pneumonia Nursing Care PlanDocument1 pageImpaired Gas Exchange Pneumonia Nursing Care Planjustin_sanePas encore d'évaluation
- NCP For PyelonephritisDocument6 pagesNCP For PyelonephritisHanna Mariel Tecson Celispara33% (3)
- Nursing Care Plan Renal FailureDocument2 pagesNursing Care Plan Renal FailureMark Jason Rabadan100% (1)
- ReportDocument4 pagesReportKyle DapulagPas encore d'évaluation
- Acute Abdominal-WPS OfficeDocument3 pagesAcute Abdominal-WPS OfficeA HPas encore d'évaluation
- Postoperative Nursing Care Plan For Cesarian Section Patient Case Pres orDocument6 pagesPostoperative Nursing Care Plan For Cesarian Section Patient Case Pres orLoren EstefanPas encore d'évaluation
- Drug Study 2Document7 pagesDrug Study 2Jediale CarcelerPas encore d'évaluation
- Practical Nursing Diploma Program Pre-Clinical Nursing Care Research Assignment "Prep and Plan"Document7 pagesPractical Nursing Diploma Program Pre-Clinical Nursing Care Research Assignment "Prep and Plan"Jeremy ThomasPas encore d'évaluation
- Subjective: IndependentDocument6 pagesSubjective: IndependentLuvdonna BorresPas encore d'évaluation
- NCP Urinary Tract InfectionDocument4 pagesNCP Urinary Tract InfectiondollythesheepPas encore d'évaluation
- NURSING CARE PLAN On LeptospirosisDocument8 pagesNURSING CARE PLAN On LeptospirosisRosalie Valdez Espiritu71% (7)
- NCP PSHDocument17 pagesNCP PSHMargareth OrtizPas encore d'évaluation
- Uti NCPDocument3 pagesUti NCPHamdy Pagilit Dimaporo0% (1)
- Nursing Care Plan For HemodialysisDocument2 pagesNursing Care Plan For Hemodialysisderic80% (20)
- Nursing Care Plan For Smoke Poisoning NCPDocument2 pagesNursing Care Plan For Smoke Poisoning NCPderic100% (3)
- Nursing Care Plan For Carbon Monoxide PoisoningDocument3 pagesNursing Care Plan For Carbon Monoxide Poisoningderic73% (11)
- Nursing Care Plan For AmputationDocument3 pagesNursing Care Plan For Amputationderic80% (25)
- Nursing Care Plan For Upper Gastrointestinal Bleeding NCPDocument3 pagesNursing Care Plan For Upper Gastrointestinal Bleeding NCPderic79% (14)
- Nursing Care Plan For Seizure NCPDocument2 pagesNursing Care Plan For Seizure NCPderic88% (40)
- Nursing Care Plan For AIDS/HIVDocument3 pagesNursing Care Plan For AIDS/HIVderic81% (16)
- Nursing Care Plan For GlaucomaDocument3 pagesNursing Care Plan For Glaucomaderic79% (28)
- Nursing Care Plan For Readiness For Enhanced Sleep NCPDocument4 pagesNursing Care Plan For Readiness For Enhanced Sleep NCPderic100% (2)
- Nursing Care Plan For Readiness For Enhanced Spiritual Well Being NCPDocument4 pagesNursing Care Plan For Readiness For Enhanced Spiritual Well Being NCPderic83% (6)
- Nursing Care Plan For Risk For Aspiration NCPDocument5 pagesNursing Care Plan For Risk For Aspiration NCPderic100% (8)
- Nursing Care Plan For Risk For Compromised Human Dignity NCPDocument3 pagesNursing Care Plan For Risk For Compromised Human Dignity NCPderic100% (2)
- Nursing Care Plan For Rape Trauma Syndrome NCPDocument5 pagesNursing Care Plan For Rape Trauma Syndrome NCPderic100% (4)
- Nursing Care Plan For Readiness For Enhanced Hope NCPDocument4 pagesNursing Care Plan For Readiness For Enhanced Hope NCPderic100% (6)
- Nursing Care Plan For Peptic Ulcer NCPDocument2 pagesNursing Care Plan For Peptic Ulcer NCPderic85% (46)
- Nursing Care Plan For Pedia TB Meningitis NCPDocument2 pagesNursing Care Plan For Pedia TB Meningitis NCPderic100% (1)
- Nursing Care Plan For Pneumonia NCPDocument3 pagesNursing Care Plan For Pneumonia NCPderic79% (133)
- Nursing Care Plan For Rabies NCPDocument3 pagesNursing Care Plan For Rabies NCPderic100% (9)
- Nursing Care Plan For Post Trauma NCPDocument5 pagesNursing Care Plan For Post Trauma NCPderic82% (11)
- Nursing Care Plan For Peritonitis NCPDocument2 pagesNursing Care Plan For Peritonitis NCPderic86% (7)
- Nursing Care Plan For Multiple Sclerosis NCPDocument2 pagesNursing Care Plan For Multiple Sclerosis NCPderic88% (17)
- Nursing Care Plan For Overflow Urinary Incontinence NCPDocument2 pagesNursing Care Plan For Overflow Urinary Incontinence NCPderic71% (7)
- Nursing Care Plan For Neonatal Sepsis NCPDocument3 pagesNursing Care Plan For Neonatal Sepsis NCPderic67% (9)
- Nursing Care Plan For Disturbed Sleep Pattern NCPDocument3 pagesNursing Care Plan For Disturbed Sleep Pattern NCPderic67% (3)
- Nursing Care Plan For Insufficient Breastmilk NCPDocument2 pagesNursing Care Plan For Insufficient Breastmilk NCPderic100% (17)
- Nursing Care Plan For Myocardial Infarction NCPDocument8 pagesNursing Care Plan For Myocardial Infarction NCPderic87% (15)
- Nursing Care Plan For Interrupted Breastfeeding NCPDocument3 pagesNursing Care Plan For Interrupted Breastfeeding NCPderic88% (8)
- Nursing Care Plan For Liver Cirrhosis NCPDocument14 pagesNursing Care Plan For Liver Cirrhosis NCPderic92% (12)
- Nursing Care Plan For Insomnia NCPDocument2 pagesNursing Care Plan For Insomnia NCPderic83% (24)
- Nursing Care Plan For Ineffective Infant Feeding Pattern NCPDocument3 pagesNursing Care Plan For Ineffective Infant Feeding Pattern NCPderic71% (14)
- The Bible Does Not Condemn Premarital SexDocument16 pagesThe Bible Does Not Condemn Premarital SexKeith502100% (3)
- Ccounting Basics and Interview Questions AnswersDocument18 pagesCcounting Basics and Interview Questions AnswersAamir100% (1)
- TLS FinalDocument69 pagesTLS FinalGrace Arthur100% (1)
- Number SystemsDocument165 pagesNumber SystemsapamanPas encore d'évaluation
- Scipaper 7Document2 pagesScipaper 7JL Serioso BalesPas encore d'évaluation
- Broshure JepanDocument6 pagesBroshure JepanIrwan Mohd YusofPas encore d'évaluation
- Defending A Dogma: Between Grice, Strawson and Quine: Elvis ImafidonDocument10 pagesDefending A Dogma: Between Grice, Strawson and Quine: Elvis ImafidonYang Wen-LiPas encore d'évaluation
- Tugas, MO - REVIEW JURNAL JIT - Ikomang Aditya Prawira Nugraha (1902612010304)Document12 pagesTugas, MO - REVIEW JURNAL JIT - Ikomang Aditya Prawira Nugraha (1902612010304)MamanxPas encore d'évaluation
- Muslim Law Full Notes 2Document32 pagesMuslim Law Full Notes 2joshi A rahulPas encore d'évaluation
- Unsolved Problems - Mathematics Edition: August 2020Document28 pagesUnsolved Problems - Mathematics Edition: August 2020Nixon LagrisolaPas encore d'évaluation
- Final Research ReportDocument14 pagesFinal Research ReportAlojado Lamuel Jesu APas encore d'évaluation
- RF Design MCQ-1Document16 pagesRF Design MCQ-1JeyavelPas encore d'évaluation
- 3er Grado - DMPA 05 - ACTIVIDAD DE COMPRENSION LECTORA - UNIT 2 - CORRECCIONDocument11 pages3er Grado - DMPA 05 - ACTIVIDAD DE COMPRENSION LECTORA - UNIT 2 - CORRECCIONANDERSON BRUCE MATIAS DE LA SOTAPas encore d'évaluation
- Sickle Cell AnemiaDocument13 pagesSickle Cell Anemiamayra100% (1)
- Air Augmented Rocket (285pages) Propulsion ConceptsDocument285 pagesAir Augmented Rocket (285pages) Propulsion ConceptsAlexandre PereiraPas encore d'évaluation
- Midterm Decision Analysis ExercisesDocument5 pagesMidterm Decision Analysis ExercisesAYLEN INJAYAPas encore d'évaluation
- MISKDocument134 pagesMISKmusyokaPas encore d'évaluation
- Brain and LanguageDocument3 pagesBrain and LanguageJasper AngelesPas encore d'évaluation
- LakmeDocument34 pagesLakmeSuraj Pratap Sawhney79% (14)
- Elementary SurveyingDocument19 pagesElementary SurveyingJefferson EscobidoPas encore d'évaluation
- Saptamsa - D7Document4 pagesSaptamsa - D7Nabeel IrfanPas encore d'évaluation
- Social Consequences of UnemploymentDocument3 pagesSocial Consequences of UnemploymentvillafuerteviPas encore d'évaluation
- Friedman LawsuitDocument12 pagesFriedman LawsuitChris GothnerPas encore d'évaluation
- Pace, ART 102, Week 6, Etruscan, Roman Arch. & SculpDocument36 pagesPace, ART 102, Week 6, Etruscan, Roman Arch. & SculpJason ByrdPas encore d'évaluation
- Electronic Load FundamentalsDocument16 pagesElectronic Load FundamentalsMiguel PenarandaPas encore d'évaluation
- Public Administration 2000 - CSS ForumsDocument3 pagesPublic Administration 2000 - CSS ForumsMansoor Ali KhanPas encore d'évaluation
- Thesis Committee MeetingDocument7 pagesThesis Committee Meetingafknojbcf100% (2)
- CHAPTER 4 (B)Document6 pagesCHAPTER 4 (B)Jon Lester De VeyraPas encore d'évaluation
- Bird Beak ActivityDocument4 pagesBird Beak Activityapi-314222661Pas encore d'évaluation
- Argumentative Essay Project DescriptionDocument5 pagesArgumentative Essay Project DescriptionKaren Jh MoncayoPas encore d'évaluation