Vous aimerez peut-être aussi
- Privatizing Medicaid in ColoradoDocument7 pagesPrivatizing Medicaid in ColoradoIndependence InstitutePas encore d'évaluation
- BPCLC Public Comment Letter in Response To The Patient Protection and Affordable Care Act Exchange Program Integrity Proposed RuleDocument5 pagesBPCLC Public Comment Letter in Response To The Patient Protection and Affordable Care Act Exchange Program Integrity Proposed RuleState Senator Liz KruegerPas encore d'évaluation
- The HMO Act of 1973 Health Maintenance Organization Act of 1973Document3 pagesThe HMO Act of 1973 Health Maintenance Organization Act of 1973Sai PrabhuPas encore d'évaluation
- ACA SummaryDocument9 pagesACA SummaryScottRobertLanePas encore d'évaluation
- Land of Lincoln Complaint in U.S. Federal Court of ClaimsDocument46 pagesLand of Lincoln Complaint in U.S. Federal Court of ClaimsCrainsChicagoBusinessPas encore d'évaluation
- The Pluralistic Reform Model: The Patient Protection and Affordable Care Act of 2010Document4 pagesThe Pluralistic Reform Model: The Patient Protection and Affordable Care Act of 2010Ben HsuPas encore d'évaluation
- Health Insurance in IndiaDocument6 pagesHealth Insurance in Indiachhavigupta1689Pas encore d'évaluation
- United States Court of Appeals: For The First CircuitDocument19 pagesUnited States Court of Appeals: For The First CircuitMetro Puerto RicoPas encore d'évaluation
- Senate Finance Committee BillDocument262 pagesSenate Finance Committee BillFOXBusiness.comPas encore d'évaluation
- Introduction To Healthcarereimbursement: Health InsuranceDocument2 pagesIntroduction To Healthcarereimbursement: Health InsurancegabigabigabrielaPas encore d'évaluation
- It's Time For A Single-Payer Healthcare System: Philip Kotler March 25, 2017Document10 pagesIt's Time For A Single-Payer Healthcare System: Philip Kotler March 25, 2017pedronuno20Pas encore d'évaluation
- StateProgramsUnderReform BriefDocument8 pagesStateProgramsUnderReform Briefkirs0069Pas encore d'évaluation
- How Is Health Care Reform Affecting U.S. Health Insurers' Market Opportunities and Risks?Document6 pagesHow Is Health Care Reform Affecting U.S. Health Insurers' Market Opportunities and Risks?api-227433089Pas encore d'évaluation
- 50 Vetoes: How States Can Stop the Obama Health Care LawD'Everand50 Vetoes: How States Can Stop the Obama Health Care LawPas encore d'évaluation
- AHM 250 Chapter 1Document9 pagesAHM 250 Chapter 1Paromita MukhopadhyayPas encore d'évaluation
- HR 1628 As PassedDocument41 pagesHR 1628 As PassedCNBC.comPas encore d'évaluation
- HEALTH INSURANCE IN INDIA: NEED, PRESENT SCENARIO AND POTENTIALDocument6 pagesHEALTH INSURANCE IN INDIA: NEED, PRESENT SCENARIO AND POTENTIALsupriyaPas encore d'évaluation
- US Health Policy and Market Reforms: An IntroductionD'EverandUS Health Policy and Market Reforms: An IntroductionPas encore d'évaluation
- New Solvency Advocate Walker 17Document4 pagesNew Solvency Advocate Walker 17saifbajwa9038Pas encore d'évaluation
- Affordable Care Act ThesisDocument5 pagesAffordable Care Act Thesisgbtrjrap100% (1)
- Backgrounder: Obamacare's Enrollment Increase: Mainly Due To Medicaid ExpansionDocument7 pagesBackgrounder: Obamacare's Enrollment Increase: Mainly Due To Medicaid ExpansionJoshua GrayPas encore d'évaluation
- Textbook of Urgent Care Management: Chapter 38, Audits by Managed-Care Organizations and Regulatory AgenciesD'EverandTextbook of Urgent Care Management: Chapter 38, Audits by Managed-Care Organizations and Regulatory AgenciesPas encore d'évaluation
- The Insider’s Guide to Obamacare’s Open Enrollment (2015-2016)D'EverandThe Insider’s Guide to Obamacare’s Open Enrollment (2015-2016)Pas encore d'évaluation
- General Commercial Health Insurance Information GuideDocument22 pagesGeneral Commercial Health Insurance Information GuideDeviselvamPas encore d'évaluation
- Newman's Medical Billing and Coding Technicians Study GuideD'EverandNewman's Medical Billing and Coding Technicians Study GuidePas encore d'évaluation
- Economic implications of medical liability claims:: Insurance and compensation schemes in EuropeD'EverandEconomic implications of medical liability claims:: Insurance and compensation schemes in EuropePas encore d'évaluation
- The Affordable Care Act's Impact On Health Insurance Ratings Is Neutral Now, But Pressure Could Build Over TimeDocument6 pagesThe Affordable Care Act's Impact On Health Insurance Ratings Is Neutral Now, But Pressure Could Build Over Timeapi-227433089Pas encore d'évaluation
- Waiver Concepts Fact SheetDocument3 pagesWaiver Concepts Fact SheetStephen LoiaconiPas encore d'évaluation
- Comments On Coventry (St. Louis) Rate Filing HIOS Issue ID #44527 1-1-16Document5 pagesComments On Coventry (St. Louis) Rate Filing HIOS Issue ID #44527 1-1-16moconsumerPas encore d'évaluation
- Medicare Update: Information To Help With The Darkness of Medicare ComplianceDocument7 pagesMedicare Update: Information To Help With The Darkness of Medicare ComplianceForge ConsultingPas encore d'évaluation
- Issue Brief 20Document7 pagesIssue Brief 20kirs0069Pas encore d'évaluation
- Comunicado Del Senado de EEUUDocument2 pagesComunicado Del Senado de EEUUTodo NoticiasPas encore d'évaluation
- Final Report For Colorado Public Option - Includes Appendices I - IVDocument101 pagesFinal Report For Colorado Public Option - Includes Appendices I - IVapi-491077033Pas encore d'évaluation
- How Is The Transition To An Exchange-Based Environment Affecting Health Insurers, Providers, and Consumers?Document5 pagesHow Is The Transition To An Exchange-Based Environment Affecting Health Insurers, Providers, and Consumers?api-227433089Pas encore d'évaluation
- Textbook of Urgent Care Management: Chapter 36, Virtual CareD'EverandTextbook of Urgent Care Management: Chapter 36, Virtual CarePas encore d'évaluation
- MEDICAL BILLING KEY TERMSDocument7 pagesMEDICAL BILLING KEY TERMSMarynaPas encore d'évaluation
- Medical Billing ProcessDocument13 pagesMedical Billing ProcessUdayaKumar100% (3)
- GAO Report On Obamacare FraudDocument58 pagesGAO Report On Obamacare FraudZerohedgePas encore d'évaluation
- Comments On United Rate Filing HIOS Issue ID #14162 1-1-16Document5 pagesComments On United Rate Filing HIOS Issue ID #14162 1-1-16moconsumerPas encore d'évaluation
- The Challenges of Medicaid Expansion Will Limit U.S. Health Insurers' Profitability in The Short TermDocument8 pagesThe Challenges of Medicaid Expansion Will Limit U.S. Health Insurers' Profitability in The Short Termapi-227433089Pas encore d'évaluation
- Mining for Gold In a Barren Land: Pioneer Accountable Care Organization Potential to Redesign the Healthcare Business Model in a Post-Acute SettingD'EverandMining for Gold In a Barren Land: Pioneer Accountable Care Organization Potential to Redesign the Healthcare Business Model in a Post-Acute SettingPas encore d'évaluation
- Compliance 2017Document5 pagesCompliance 2017Swisskelly1Pas encore d'évaluation
- HR Guide to Surviving Health ReformDocument4 pagesHR Guide to Surviving Health ReformMuhammad UsmanPas encore d'évaluation
- State Health Exchanges and Qualified Health PlansDocument49 pagesState Health Exchanges and Qualified Health PlansRajiv GargPas encore d'évaluation
- Health Affairs: For Reprints, Links & PermissionsDocument17 pagesHealth Affairs: For Reprints, Links & Permissionsmick84Pas encore d'évaluation
- Health Insurance: Passed By: Rhea May PoriloDocument12 pagesHealth Insurance: Passed By: Rhea May PoriloRhea May PoriloPas encore d'évaluation
- The Affordable Care ActDocument7 pagesThe Affordable Care ActalexPas encore d'évaluation
- Newman's Billing and Coding Technicians Study GuideD'EverandNewman's Billing and Coding Technicians Study GuideÉvaluation : 4.5 sur 5 étoiles4.5/5 (2)
- CEO Talking Points On Risk Corridor RepealDocument1 pageCEO Talking Points On Risk Corridor RepealChris GeidnerPas encore d'évaluation
- 1.evolution of Heath PlansDocument9 pages1.evolution of Heath PlansUtpal Kumar PalPas encore d'évaluation
- AHM 250 Course MaterialDocument285 pagesAHM 250 Course MaterialAnitha Viji73% (15)
- Obamacare OrderDocument29 pagesObamacare OrderRoger DuPuisPas encore d'évaluation
- The Costs of Regulation and Centralization in Health Care by Scott AtlasDocument22 pagesThe Costs of Regulation and Centralization in Health Care by Scott AtlasHoover InstitutionPas encore d'évaluation
- Healthcare TerminologiesDocument26 pagesHealthcare Terminologiesitsme itsmePas encore d'évaluation
- RSC S Surprise Medical Billing Backgrounder.02Document8 pagesRSC S Surprise Medical Billing Backgrounder.02Peter SullivanPas encore d'évaluation
- 2020 BizWomen BioBookDocument16 pages2020 BizWomen BioBookPortland Business JournalPas encore d'évaluation
- ORLA ComplaintDocument5 pagesORLA ComplaintPortland Business JournalPas encore d'évaluation
- Benchmade v. HogueDocument13 pagesBenchmade v. HoguePortland Business JournalPas encore d'évaluation
- Mayor Wheeler Police Reform Action Plan June 9 2020Document2 pagesMayor Wheeler Police Reform Action Plan June 9 2020Portland Business JournalPas encore d'évaluation
- 2016 Kauffman Startup Index - MetroDocument72 pages2016 Kauffman Startup Index - MetroPortland Business JournalPas encore d'évaluation
- 88 18 Legacy Good Sam NOIDocument16 pages88 18 Legacy Good Sam NOIPortland Business JournalPas encore d'évaluation
- PBJ CrosswordDocument1 pagePBJ CrosswordPortland Business Journal0% (1)
- 2020 BizWomen BioBook - 021420Document14 pages2020 BizWomen BioBook - 021420Portland Business JournalPas encore d'évaluation
- 2020 BizWomen BioBook - 021320Document14 pages2020 BizWomen BioBook - 021320Portland Business JournalPas encore d'évaluation
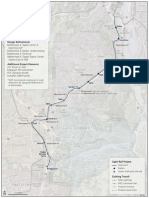
- Southwest Corridor MapDocument1 pageSouthwest Corridor MapPortland Business JournalPas encore d'évaluation
- USA v. Gatto Opening StatementsDocument87 pagesUSA v. Gatto Opening StatementsPortland Business JournalPas encore d'évaluation
- TechTown Survey Data 2016Document20 pagesTechTown Survey Data 2016Portland Business JournalPas encore d'évaluation
- ComplaintDocument14 pagesComplaintPortland Business JournalPas encore d'évaluation
- Merkley Lawsuit To Halt Kavanaugh Confirmation ProcessDocument28 pagesMerkley Lawsuit To Halt Kavanaugh Confirmation ProcessKGW NewsPas encore d'évaluation
- Class and Collective Action Allegation Complaint-Dkt 1Document43 pagesClass and Collective Action Allegation Complaint-Dkt 1Portland Business JournalPas encore d'évaluation
- PPSs Response To Letter of Intent Fro M Macadam Forbes - Final - April 27Document1 pagePPSs Response To Letter of Intent Fro M Macadam Forbes - Final - April 27Portland Business JournalPas encore d'évaluation
- Intel WARN Oregon Letter April 2016Document2 pagesIntel WARN Oregon Letter April 2016Portland Business JournalPas encore d'évaluation
- Seaport Airlines Reorganization PlanDocument75 pagesSeaport Airlines Reorganization PlanPortland Business JournalPas encore d'évaluation
- Hattar/Huffman Complaint Filed 5-16-16 - Case No. 16-cv-16090 (00296335x9C8DB)Document28 pagesHattar/Huffman Complaint Filed 5-16-16 - Case No. 16-cv-16090 (00296335x9C8DB)Portland Business JournalPas encore d'évaluation
- Lawsuit Filed To Stop Portland From Allowing Homeless CampsDocument15 pagesLawsuit Filed To Stop Portland From Allowing Homeless CampsPortland Business JournalPas encore d'évaluation
- Appendix 1: List of Potentially Regulated Entities: Fossil Fuel SuppliersDocument5 pagesAppendix 1: List of Potentially Regulated Entities: Fossil Fuel SuppliersPortland Business JournalPas encore d'évaluation
- Portland Arts Tax Ruling June 8, 2016Document12 pagesPortland Arts Tax Ruling June 8, 2016Portland Business JournalPas encore d'évaluation
- Ertischek V ViewpointDocument23 pagesErtischek V ViewpointPortland Business JournalPas encore d'évaluation
- Firstsource EugeneDocument2 pagesFirstsource EugenePortland Business JournalPas encore d'évaluation
- FERC Jordan Cove Coos BayDocument25 pagesFERC Jordan Cove Coos BayPortland Business JournalPas encore d'évaluation
- SEC Aequitas ComplaintDocument30 pagesSEC Aequitas ComplaintPortland Business JournalPas encore d'évaluation
- Letter From Oracle To Sec. BurwellDocument47 pagesLetter From Oracle To Sec. BurwellPortland Business JournalPas encore d'évaluation
- State of Oregon Comments On Federal Health Exchange Program 3 Percent TaxDocument12 pagesState of Oregon Comments On Federal Health Exchange Program 3 Percent TaxPortland Business JournalPas encore d'évaluation
- Providence Merger NotesDocument21 pagesProvidence Merger NotesPortland Business JournalPas encore d'évaluation
- Adarne Vs AldbabaDocument3 pagesAdarne Vs AldbabaKimberly TimtimPas encore d'évaluation
- Awesome Civ Pro OutlineDocument78 pagesAwesome Civ Pro Outlinebeenishzahid100% (1)
- PDS Additional SheetDocument3 pagesPDS Additional SheetJonathan BautistaPas encore d'évaluation
- CIBIL Consent FormDocument4 pagesCIBIL Consent FormKuldeep BatraPas encore d'évaluation
- Bisset and Others V Boland Bank LTD and Others 1991 (4) Sa 603 (D)Document9 pagesBisset and Others V Boland Bank LTD and Others 1991 (4) Sa 603 (D)Rodney UlyatePas encore d'évaluation
- Member Design - Reinforced Concrete Staircase BS8110 v2017.01Document78 pagesMember Design - Reinforced Concrete Staircase BS8110 v2017.01sreejit77Pas encore d'évaluation
- IPR II - 3yr LLBDocument78 pagesIPR II - 3yr LLBGRKPas encore d'évaluation
- Malaysian Spectrum Licensing Framework - Stella Jeevamani NavaratnamDocument23 pagesMalaysian Spectrum Licensing Framework - Stella Jeevamani NavaratnamRazman RashidPas encore d'évaluation
- Phool Patti and Anr Vs Ram Singh (Dead) Through Lrs. & Anr On 6 January, 2015Document7 pagesPhool Patti and Anr Vs Ram Singh (Dead) Through Lrs. & Anr On 6 January, 2015sreeranganPas encore d'évaluation
- Thermodynamics Take Home QuizDocument3 pagesThermodynamics Take Home QuizMichael QuidorPas encore d'évaluation
- Your Document Checklist - Immigration, Refugees and Citizenship Canada PDFDocument2 pagesYour Document Checklist - Immigration, Refugees and Citizenship Canada PDFcreadorcitoPas encore d'évaluation
- SMART Meter Refusal LetterDocument11 pagesSMART Meter Refusal Letterfree100% (1)
- Alawiya V Court of Appeals, GR No. 164170, April 16, 2009Document1 pageAlawiya V Court of Appeals, GR No. 164170, April 16, 2009Lyle BucolPas encore d'évaluation
- IRS InfoDocument4 pagesIRS InfoClint Clinton100% (1)
- SPOUSES EsmaquelDocument1 pageSPOUSES EsmaquelMonalizts D.Pas encore d'évaluation
- Letters of Intent in ConstructionDocument4 pagesLetters of Intent in ConstructionSursarovar50% (2)
- Clean Air Act of 1999 and Solid Waste Management Act of 2000Document43 pagesClean Air Act of 1999 and Solid Waste Management Act of 2000AcelojoPas encore d'évaluation
- RTIDocument2 pagesRTIVibin NairPas encore d'évaluation
- KTT 55 - 45 20230622 Wa0013. 6 2 - 082636 1Document13 pagesKTT 55 - 45 20230622 Wa0013. 6 2 - 082636 1Mahi AkhtarPas encore d'évaluation
- Suggested Answers For Political Law Mock Bar ExamDocument5 pagesSuggested Answers For Political Law Mock Bar ExamMikez NazalPas encore d'évaluation
- Singing The Past: Vietnamese Ca Tru, Memory, and ModeDocument31 pagesSinging The Past: Vietnamese Ca Tru, Memory, and ModePhung Ha ThanhPas encore d'évaluation
- Clarifying DILG Memo on Eviction, Demolition RequirementsDocument3 pagesClarifying DILG Memo on Eviction, Demolition RequirementsAnonymous Td8oR1s7DPas encore d'évaluation
- Maryland Property Associates v. Colombo Bank, 4th Cir. (2009)Document37 pagesMaryland Property Associates v. Colombo Bank, 4th Cir. (2009)Scribd Government DocsPas encore d'évaluation
- Supply and Delivery of Various Construction Materials For PHSIDocument3 pagesSupply and Delivery of Various Construction Materials For PHSIWestern Mindanao State UniversityPas encore d'évaluation
- Does Death Extinguish Civil Liability for CrimesDocument2 pagesDoes Death Extinguish Civil Liability for CrimesranaalyssagmailcomPas encore d'évaluation
- IRCTC travel insurance coverDocument3 pagesIRCTC travel insurance coverAbhinav TayadePas encore d'évaluation
- United States v. Jerome Fields, 833 F.2d 1006, 4th Cir. (1987)Document2 pagesUnited States v. Jerome Fields, 833 F.2d 1006, 4th Cir. (1987)Scribd Government DocsPas encore d'évaluation
- Fraternity Waiver Contract RulesDocument1 pageFraternity Waiver Contract RulesCham TenorioPas encore d'évaluation
- JNTUK B.Tech R16 RegulationsDocument13 pagesJNTUK B.Tech R16 RegulationsSrinidhi A BelieverPas encore d'évaluation
- 30 (B) Mathematics For (Blind)Document15 pages30 (B) Mathematics For (Blind)REHAN ALAMPas encore d'évaluation