Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Fall Prevention PosterDocument1 pageFall Prevention Posterapi-241173284Pas encore d'évaluation
- Refusal To Vaccinate FormDocument1 pageRefusal To Vaccinate FormblcksourcePas encore d'évaluation
- Steranios 2 - Steranios 2 - NG Steranios 2 - ECS Fiche Technique 00000 enDocument2 pagesSteranios 2 - Steranios 2 - NG Steranios 2 - ECS Fiche Technique 00000 enbiomedico gastroadvancedPas encore d'évaluation
- Serological Classification of BacteriaDocument16 pagesSerological Classification of BacteriaThe Apollo ClinicPas encore d'évaluation
- Measles PamphletDocument2 pagesMeasles Pamphletapi-384459604Pas encore d'évaluation
- BioSARSCov2 StudentDocument5 pagesBioSARSCov2 StudentMedardo Sabillon MedinaPas encore d'évaluation
- Helen Mcdonald Case Study 1Document24 pagesHelen Mcdonald Case Study 1api-241173284Pas encore d'évaluation
- Helen Mcdonald Case Study 2Document21 pagesHelen Mcdonald Case Study 2api-241173284Pas encore d'évaluation
- Harrington R Mcdonald H 2016 Parkinsons Disease State University of New York Polytechnic InstituteDocument32 pagesHarrington R Mcdonald H 2016 Parkinsons Disease State University of New York Polytechnic Instituteapi-241173284Pas encore d'évaluation
- Mcdonald H Harrington R 2015 Childhood Obesity Community Teaching Project FinalDocument10 pagesMcdonald H Harrington R 2015 Childhood Obesity Community Teaching Project Finalapi-241173284Pas encore d'évaluation
- Helen Mcdonald Case Study 1Document20 pagesHelen Mcdonald Case Study 1api-241173284Pas encore d'évaluation
- Values ConflictDocument3 pagesValues Conflictapi-241173284Pas encore d'évaluation
- Helen Mcdonald Family Theory Final Paper Nur531Document10 pagesHelen Mcdonald Family Theory Final Paper Nur531api-241173284Pas encore d'évaluation
- Nur 455 Public Health Project 2Document30 pagesNur 455 Public Health Project 2api-241173284Pas encore d'évaluation
- Rosario IPCRDocument32 pagesRosario IPCRSaephan MariePas encore d'évaluation
- Ethical Issues-Case StudiesDocument7 pagesEthical Issues-Case StudiesMelissa RobinsonPas encore d'évaluation
- COVID-19 Prevention and Control Quarantine and Border Control ProtocolDocument4 pagesCOVID-19 Prevention and Control Quarantine and Border Control ProtocolTsehaye yonasPas encore d'évaluation
- Acute Tonsillopharyngitis - NonexudativeDocument12 pagesAcute Tonsillopharyngitis - NonexudativeLemuel GuevarraPas encore d'évaluation
- Bacterial Sinusitis in Children: AcuteDocument11 pagesBacterial Sinusitis in Children: AcutefriscahalimPas encore d'évaluation
- EUCAST Quality Check TablesDocument20 pagesEUCAST Quality Check TableswitoldPas encore d'évaluation
- Handling & Animal Restraint of Laboratory Test Animals: Definition of Terms: Definition of TermsDocument14 pagesHandling & Animal Restraint of Laboratory Test Animals: Definition of Terms: Definition of TermsFrances SaludPas encore d'évaluation
- ShingrixDocument6 pagesShingrixMarcus YoonPas encore d'évaluation
- Czech Republic Doctors Have Founded A Parallel Medical AssociationDocument3 pagesCzech Republic Doctors Have Founded A Parallel Medical AssociationsylodhiPas encore d'évaluation
- Tattoo Studios RegulationDocument15 pagesTattoo Studios RegulationPanama Inked AkiPas encore d'évaluation
- Cvs 10878Document7 pagesCvs 10878jwilliams_335176Pas encore d'évaluation
- Anti Rabies CampaignDocument3 pagesAnti Rabies CampaignJoey YusingcoPas encore d'évaluation
- Indonesia National Immunization Program:: Dr. Prima Yosephine Epi Manager Moh IndonesiaDocument19 pagesIndonesia National Immunization Program:: Dr. Prima Yosephine Epi Manager Moh IndonesiaAstri KhairanaPas encore d'évaluation
- Nabh - HRDocument10 pagesNabh - HRUtsab BagchiPas encore d'évaluation
- Mohap Uae Registered Parenteral Form of Medication (Injections)Document2 091 pagesMohap Uae Registered Parenteral Form of Medication (Injections)jaad vanimalPas encore d'évaluation
- Vaccines and Related Biological Products Advisory Committee MeetingDocument64 pagesVaccines and Related Biological Products Advisory Committee MeetingJim HoftPas encore d'évaluation
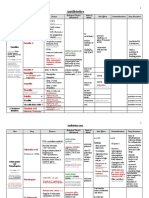
- Antimicrobial Drugs TableDocument19 pagesAntimicrobial Drugs TableLaylee ClarePas encore d'évaluation
- Isolasi Dan Kultivasi MikroorganismeDocument27 pagesIsolasi Dan Kultivasi MikroorganismeRahma NabilaPas encore d'évaluation
- Outbreak Investigation Part 1 PDFDocument4 pagesOutbreak Investigation Part 1 PDFashythegreat93Pas encore d'évaluation
- Hepatitis B: Pathophysiology and TransmissionDocument6 pagesHepatitis B: Pathophysiology and TransmissionEndrianus Jaya PutraPas encore d'évaluation
- Cable Abbreviations With Woven Cable PatternDocument2 pagesCable Abbreviations With Woven Cable PatterntritidiefPas encore d'évaluation
- Malaria 2Document1 pageMalaria 2jvPas encore d'évaluation
- Streptococcus Pneumoniae: Pathogenesis and DiseaseDocument10 pagesStreptococcus Pneumoniae: Pathogenesis and DiseaseAlistair LauPas encore d'évaluation
- Community Health NursingDocument36 pagesCommunity Health Nursingglen100% (1)
- Parents' Knowledge, Attitude, and Practice On Childhood ImmunizationDocument7 pagesParents' Knowledge, Attitude, and Practice On Childhood ImmunizationUlil Amri PramadaniPas encore d'évaluation