Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Social Justice Final ReflectionDocument2 pagesSocial Justice Final Reflectionapi-310815315Pas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Evidence Based Final ReflectionDocument2 pagesEvidence Based Final Reflectionapi-310815315Pas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Leadership Final ReflectionDocument2 pagesLeadership Final Reflectionapi-310815315Pas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- 645 Home Eval Summary Phi EdittedDocument15 pages645 Home Eval Summary Phi Edittedapi-310815315Pas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- 660 Midterm Level II EvalDocument8 pages660 Midterm Level II Evalapi-310815315Pas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- 660 Final Level II EvaluationDocument7 pages660 Final Level II Evaluationapi-310815315Pas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Submitted My BrandDocument2 pagesSubmitted My Brandapi-310815315Pas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- 630 Submitted Occupational Profile and AnalysisDocument21 pages630 Submitted Occupational Profile and Analysisapi-310815315Pas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- PediatricsDocument3 pagesPediatricsapi-291545292Pas encore d'évaluation
- Resume February 2016Document1 pageResume February 2016api-310815315Pas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- PediatricsDocument3 pagesPediatricsapi-291545292Pas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- PediatricsDocument3 pagesPediatricsapi-291545292Pas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- 508 Developement Professional GoalspdfDocument4 pages508 Developement Professional Goalspdfapi-310815315Pas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Poverty PPT Final X 2Document38 pagesPoverty PPT Final X 2api-293243330Pas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Oncology Ot Use by Older Adults With CancerDocument11 pagesOncology Ot Use by Older Adults With Cancerapi-310815315Pas encore d'évaluation
- Occupational Therapy Activities and Intervention Techniques For Clients With Stroke in Six Rehabilitation Hospitals - 2006 - 369Document10 pagesOccupational Therapy Activities and Intervention Techniques For Clients With Stroke in Six Rehabilitation Hospitals - 2006 - 369BeatrizIgelmoPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- 651 Submitted Occupational ProfileDocument20 pages651 Submitted Occupational Profileapi-310815315Pas encore d'évaluation
- 660 Research ArticlesDocument2 pages660 Research Articlesapi-310815315Pas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- 526 Child-Based Pico ResearchDocument7 pages526 Child-Based Pico Researchapi-310815315Pas encore d'évaluation
- Case StudyDocument23 pagesCase Studyapi-282753416Pas encore d'évaluation
- 649 Assistive Technology PaperDocument8 pages649 Assistive Technology Paperapi-310815315Pas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- 506 Occupational Analysis Intervention Plan CompletedDocument20 pages506 Occupational Analysis Intervention Plan Completedapi-310815315Pas encore d'évaluation
- Scholarly Work - Qualitative ResearchDocument12 pagesScholarly Work - Qualitative Researchapi-292815157Pas encore d'évaluation
- Quantitative PaperDocument10 pagesQuantitative Paperapi-292815157Pas encore d'évaluation
- Submitted Cat PaperDocument12 pagesSubmitted Cat Paperapi-310815315Pas encore d'évaluation
- School of Occupational Therapy Touro University Nevada OCCT 643 Systematic Reviews in Occupational Therapy Critically Appraised Topic ProjectDocument19 pagesSchool of Occupational Therapy Touro University Nevada OCCT 643 Systematic Reviews in Occupational Therapy Critically Appraised Topic Projectapi-310815315Pas encore d'évaluation
- Jurnal Ketepatan Kode Ketileng PDFDocument14 pagesJurnal Ketepatan Kode Ketileng PDFDiah Ayu KartikasariPas encore d'évaluation
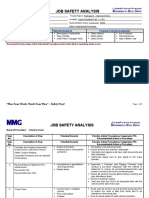
- Travelling of CraneDocument3 pagesTravelling of CraneDelta akathehuskyPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Oup Accepted Manuscript 2017 PDFDocument8 pagesOup Accepted Manuscript 2017 PDFatikha apriliaPas encore d'évaluation
- PICOT QuestionDocument1 pagePICOT Questionmelodia gandezaPas encore d'évaluation
- Med Writing 5Document4 pagesMed Writing 5dr.alicePas encore d'évaluation
- Renal Artery Stenosis Treatment Consumer GuideDocument8 pagesRenal Artery Stenosis Treatment Consumer GuideAHRQEHCProgramPas encore d'évaluation
- Pharmacological Review of AnticoagulantsDocument16 pagesPharmacological Review of AnticoagulantsDiplomski Seminarski RadoviPas encore d'évaluation
- Dream Job EssayDocument4 pagesDream Job Essaysirthana697547Pas encore d'évaluation
- Disability ManagementDocument346 pagesDisability Managementsollu786_889163149Pas encore d'évaluation
- Bill No Date Issued by Towards Amount (RS)Document4 pagesBill No Date Issued by Towards Amount (RS)mm8871Pas encore d'évaluation
- 03.2 2022ed NDTerminologySheetDocument3 pages03.2 2022ed NDTerminologySheetWidhyPas encore d'évaluation
- The British High Commission Is An Equal Opportunity EmployerDocument4 pagesThe British High Commission Is An Equal Opportunity EmployerFahim John BhattiPas encore d'évaluation
- Homework 6: I. Recognize The Mistakes and Correct ThemDocument4 pagesHomework 6: I. Recognize The Mistakes and Correct ThemTiến Lê MạnhPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- OSH 310 Readings Enviromental HealthDocument134 pagesOSH 310 Readings Enviromental Healthizzyklin23Pas encore d'évaluation
- Bsmmu DDV Curriculum 2012 New EdDocument18 pagesBsmmu DDV Curriculum 2012 New Edshahed100% (1)
- Hiv-Aids Workplace Policy and ProgramDocument4 pagesHiv-Aids Workplace Policy and ProgramluckyPas encore d'évaluation
- Cardiac Arrestin Pregnancy AScientific Statement Fromthe American HeaDocument28 pagesCardiac Arrestin Pregnancy AScientific Statement Fromthe American HeaАнђела КостићPas encore d'évaluation
- Common Psychiatric Symptoms and Key Terms in Psychiatric NursingDocument3 pagesCommon Psychiatric Symptoms and Key Terms in Psychiatric NursingQueeny Anne ApilPas encore d'évaluation
- DK Memory Activity BookDocument226 pagesDK Memory Activity Bookasif dxb100% (2)
- Guide To Interpreting MicsDocument4 pagesGuide To Interpreting MicsVlad VladPas encore d'évaluation
- AnaemiaDocument43 pagesAnaemiaMy NamePas encore d'évaluation
- Social Media Impact On Teens Issue Exploration Essay EnglishDocument4 pagesSocial Media Impact On Teens Issue Exploration Essay Englishapi-534589457Pas encore d'évaluation
- Maria Leah J. Preglo, Sharina Caranzo Calvadores, Rose Ann B. Gayon, Mildred M. Mustausa, Aris Rex D. Espinas, and Irah Vone P. AlfecheDocument10 pagesMaria Leah J. Preglo, Sharina Caranzo Calvadores, Rose Ann B. Gayon, Mildred M. Mustausa, Aris Rex D. Espinas, and Irah Vone P. AlfechedawnPas encore d'évaluation
- Week 2Document2 pagesWeek 2Francyne Jhayda EspañolaPas encore d'évaluation
- Avrutavata and Its ChikitsaDocument3 pagesAvrutavata and Its ChikitsaSamhitha Ayurvedic ChennaiPas encore d'évaluation
- Teachers Best Practices in Teaching Kindergarten Pupils An Approach To Framework ImplementationDocument13 pagesTeachers Best Practices in Teaching Kindergarten Pupils An Approach To Framework ImplementationIOER International Multidisciplinary Research Journal ( IIMRJ)Pas encore d'évaluation
- Neonatal MortalityDocument8 pagesNeonatal MortalityGlady Jane TevesPas encore d'évaluation
- A Case Report Using Regenerative Therapy For Generalized Aggressive PeriodontitisDocument9 pagesA Case Report Using Regenerative Therapy For Generalized Aggressive PeriodontitisripadiPas encore d'évaluation
- Health Risks of GMODocument3 pagesHealth Risks of GMONursita Galih PermatasariPas encore d'évaluation
- Quezon City - Ang Tahanan NG Quezon City3Document11 pagesQuezon City - Ang Tahanan NG Quezon City3Jalimay CabadingPas encore d'évaluation
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDD'EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDÉvaluation : 4.5 sur 5 étoiles4.5/5 (167)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryD'EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryÉvaluation : 4.5 sur 5 étoiles4.5/5 (157)
- An Autobiography of Trauma: A Healing JourneyD'EverandAn Autobiography of Trauma: A Healing JourneyÉvaluation : 5 sur 5 étoiles5/5 (2)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisD'EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (9)