Vous aimerez peut-être aussi
- Beginning Shift BaselineDocument1 pageBeginning Shift Baselineapi-302708069Pas encore d'évaluation
- Time Laboratory Test Collection Tube 0600Document1 pageTime Laboratory Test Collection Tube 0600api-302708069Pas encore d'évaluation
- Va AlgorithmDocument1 pageVa Algorithmapi-302708069Pas encore d'évaluation
- Elso Anticoagulation Guideline 8-2014-Table-Contents 1Document17 pagesElso Anticoagulation Guideline 8-2014-Table-Contents 1api-302708069Pas encore d'évaluation
- Blood FlowDocument1 pageBlood Flowapi-302708069Pas encore d'évaluation
- Khaja 2010 Am J Clini PatholDocument5 pagesKhaja 2010 Am J Clini Patholapi-302708069Pas encore d'évaluation
- VV Algorithm 2012Document1 pageVV Algorithm 2012api-302708069Pas encore d'évaluation
- Brain ImageryDocument1 pageBrain Imageryapi-302708069Pas encore d'évaluation
- EcprDocument9 pagesEcprapi-302708069Pas encore d'évaluation
- Nankervis 2007 Asaio Antixa-Heparin-ActsDocument4 pagesNankervis 2007 Asaio Antixa-Heparin-Actsapi-302708069Pas encore d'évaluation
- London Uk Guys Hosp New Anticoag EcmoDocument3 pagesLondon Uk Guys Hosp New Anticoag Ecmoapi-302708069Pas encore d'évaluation
- Oliver 2009 Nice OverviewDocument23 pagesOliver 2009 Nice Overviewapi-302708069Pas encore d'évaluation
- Ecmo Bsi Abstract FinalDocument1 pageEcmo Bsi Abstract Finalapi-302708069Pas encore d'évaluation
- Elso - HMNV Bronchiolitis FinalDocument1 pageElso - HMNV Bronchiolitis Finalapi-302708069Pas encore d'évaluation
- Vad - Emergency De-Airing Centrimag 2015Document4 pagesVad - Emergency De-Airing Centrimag 2015api-302708069Pas encore d'évaluation
- Eclscircsim 2011 Edit 3Document10 pagesEclscircsim 2011 Edit 3api-302708069Pas encore d'évaluation
- Co-Straight Connector With LL Change-Out 2013Document2 pagesCo-Straight Connector With LL Change-Out 2013api-302708069Pas encore d'évaluation
- External Drive Failure 2013Document2 pagesExternal Drive Failure 2013api-302708069Pas encore d'évaluation
- Co-Connectors 2013Document2 pagesCo-Connectors 2013api-302708069Pas encore d'évaluation
- Co-Entire Bridge Tubing and y ConnectorsDocument2 pagesCo-Entire Bridge Tubing and y Connectorsapi-302708069Pas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- AL PREPARE Advance Directive EnglishDocument15 pagesAL PREPARE Advance Directive EnglishSPas encore d'évaluation
- Run Report Generic TemplateDocument2 pagesRun Report Generic TemplatemeljamerlanPas encore d'évaluation
- Adult CPR GuidelinesDocument1 pageAdult CPR GuidelinesMarta Hrynyovska100% (2)
- Emergency Management of Severe BurnsDocument97 pagesEmergency Management of Severe BurnsAyu SyartikaPas encore d'évaluation
- CPR: Life-Saving Skills for Cardiac EmergenciesDocument19 pagesCPR: Life-Saving Skills for Cardiac EmergenciesNidhi KaushalPas encore d'évaluation
- Standard operating procedure for collapsed inpatientsDocument6 pagesStandard operating procedure for collapsed inpatientsAnggriawanCaesarNurfattah100% (1)
- Emergency Medical Responder - First On Scene (PDFDrive)Document656 pagesEmergency Medical Responder - First On Scene (PDFDrive)Diego Armando Castro100% (3)
- CPR and Airway Mgt.Document26 pagesCPR and Airway Mgt.Pierenne Virgil Suarez PinlacPas encore d'évaluation
- FHSAA PolicyDocument11 pagesFHSAA PolicyABC Action NewsPas encore d'évaluation
- CPR ReportingDocument39 pagesCPR ReportingNheler SonPas encore d'évaluation
- AlHawasi - Manual of Clinical PediatricDocument276 pagesAlHawasi - Manual of Clinical PediatricAhmad Just100% (2)
- BleedingDocument3 pagesBleedingNor FarehaPas encore d'évaluation
- Hesi RN Exit Exam V3Document37 pagesHesi RN Exit Exam V3Eniti100% (1)
- Unit 10: Safety First: Lessons 1 & 2: GrammarDocument12 pagesUnit 10: Safety First: Lessons 1 & 2: GrammarFABIOLA MALLAPas encore d'évaluation
- NABH FAQ'sDocument16 pagesNABH FAQ'sarun8591100% (1)
- Ccypi 3.0Document76 pagesCcypi 3.0GirishPas encore d'évaluation
- Rescue 1122 NTS /PTS Test Preparation GuideDocument47 pagesRescue 1122 NTS /PTS Test Preparation GuideLovely JuttPas encore d'évaluation
- Steps in First Aid: Emergency Action Principle: Training Packages For Health EmergenciesDocument18 pagesSteps in First Aid: Emergency Action Principle: Training Packages For Health Emergenciesruiza corcinoPas encore d'évaluation
- Capnography: Dr. Jacqueline D'Mello Dr. Manju ButaniDocument10 pagesCapnography: Dr. Jacqueline D'Mello Dr. Manju ButaniMarco Morante VegaPas encore d'évaluation
- Escort ResumeDocument7 pagesEscort Resumesyn0tiwemym3100% (2)
- P.E 3 (Individual, Dual, First Aid and Water Safety)Document42 pagesP.E 3 (Individual, Dual, First Aid and Water Safety)Lara Jean NacionalesPas encore d'évaluation
- DynaMotive BioOil BookDocument21 pagesDynaMotive BioOil BookTJBPas encore d'évaluation
- Prometric Nurse-2Document89 pagesPrometric Nurse-2AHAMED SHIFAANPas encore d'évaluation
- Bachelor of Science in Nursing: Care of Mother and Child and AdolescentDocument12 pagesBachelor of Science in Nursing: Care of Mother and Child and AdolescentJaja ManezPas encore d'évaluation
- Fseast Event HandbookDocument31 pagesFseast Event HandbookDomiiiPas encore d'évaluation
- Capnography/ End-Tidal CO Monitoring: Optional, Advanced EMTDocument14 pagesCapnography/ End-Tidal CO Monitoring: Optional, Advanced EMTMark ReinhardtPas encore d'évaluation
- Understanding Early Warning Scoring Systems (EWSSDocument50 pagesUnderstanding Early Warning Scoring Systems (EWSSDian Nurizmaisyaf100% (1)
- ACLS Cheat SheetDocument8 pagesACLS Cheat SheetLenTheRN85% (27)
- AHA On-Call PackagesDocument5 pagesAHA On-Call PackagesaliahPas encore d'évaluation
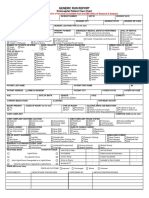
- Generic Run Report: Prehospital Patient Care ChartDocument2 pagesGeneric Run Report: Prehospital Patient Care ChartBCF PRODUCTIONPas encore d'évaluation