Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Corrective Exercise ChartDocument7 pagesCorrective Exercise ChartHrishant100% (6)
- 16 Week Athletic Domination ProgramDocument56 pages16 Week Athletic Domination ProgramShuo Zheng100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Vocabulary Graphic Organizers For LearningDocument18 pagesVocabulary Graphic Organizers For Learningapi-290467011Pas encore d'évaluation
- Wendler 5-3-1Document36 pagesWendler 5-3-1drew58Pas encore d'évaluation
- The BarBend Gun-Growing GuideDocument29 pagesThe BarBend Gun-Growing Guideft8jzh99wmPas encore d'évaluation
- Best Way To Increase StaminaDocument30 pagesBest Way To Increase StaminaSatish Kumar DashPas encore d'évaluation
- 22-0009 Robert A. Baffert - Class CDocument1 page22-0009 Robert A. Baffert - Class CMatthew StahlPas encore d'évaluation
- Grammar There Is - There AreDocument1 pageGrammar There Is - There ArerafaelaPas encore d'évaluation
- Boucher v. Syracuse University, 164 F.3d 113, 2d Cir. (1999)Document10 pagesBoucher v. Syracuse University, 164 F.3d 113, 2d Cir. (1999)Scribd Government DocsPas encore d'évaluation
- GZCLPDocument14 pagesGZCLPAlex ThomasPas encore d'évaluation
- BMX Street Bikes BikesDocument10 pagesBMX Street Bikes Bikesatif ahmedPas encore d'évaluation
- MYOLOGYDocument20 pagesMYOLOGYNatty ChikumbaPas encore d'évaluation
- Ramri Khar A Ni Chungin Ramri-A Duty Ten Bungrua Nuai 3 Chuang Man Hu Man TawhDocument2 pagesRamri Khar A Ni Chungin Ramri-A Duty Ten Bungrua Nuai 3 Chuang Man Hu Man TawhChcha VartePas encore d'évaluation
- Arrotondamento: Calf RaisesDocument4 pagesArrotondamento: Calf RaisesFederico GennariPas encore d'évaluation
- History of FIFADocument2 pagesHistory of FIFAankitabhat93Pas encore d'évaluation
- Coe68 Malang PDFDocument20 pagesCoe68 Malang PDFBhagas KaraPas encore d'évaluation
- RTS BR 25 M WrabfDocument18 pagesRTS BR 25 M WrabfEdi IrawanPas encore d'évaluation
- PlayerDocument246 pagesPlayerronhoPas encore d'évaluation
- Bubble Sports Complex Covid19 SOPDocument5 pagesBubble Sports Complex Covid19 SOPjoshPas encore d'évaluation
- Football BrochureDocument60 pagesFootball Brochurembowman18765Pas encore d'évaluation
- World Cup Soccer OPS TextDocument152 pagesWorld Cup Soccer OPS TextRod ClemenPas encore d'évaluation
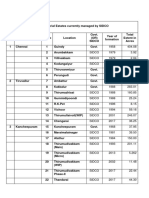
- 118 Industrial Estates Managed by SIDCODocument5 pages118 Industrial Estates Managed by SIDCODhana SekarPas encore d'évaluation
- 03 Zinn V ParrishDocument7 pages03 Zinn V ParrishBeau MasiglatPas encore d'évaluation
- Adventure Guide To AntiguaDocument258 pagesAdventure Guide To AntiguaMarcep PuscasPas encore d'évaluation
- History of Pool 1960-1969Document120 pagesHistory of Pool 1960-1969Deno J. AndrewsPas encore d'évaluation
- Indiabulls Centrum Park Luxury Homes GurgaonDocument10 pagesIndiabulls Centrum Park Luxury Homes GurgaonAsh ShuklaPas encore d'évaluation
- T, 1-2 Ipe, 1-2 Hem, 1-2 Heb, 1-2 HeaDocument46 pagesT, 1-2 Ipe, 1-2 Hem, 1-2 Heb, 1-2 HeaCédric ConreuxPas encore d'évaluation
- A Step Towards Improving Ncho Traditional Game in Anambra StateDocument3 pagesA Step Towards Improving Ncho Traditional Game in Anambra StatetheijesPas encore d'évaluation
- Giant Bicycles Bike 1249Document1 pageGiant Bicycles Bike 1249Andrés Criollo FarfánPas encore d'évaluation
- Reading: A) Carl Lewis Was Born On July 1. 1961 inDocument3 pagesReading: A) Carl Lewis Was Born On July 1. 1961 inYektiningtiasPas encore d'évaluation