Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- EMR Documentation TemplatesDocument25 pagesEMR Documentation TemplatesFlint Ray100% (1)
- Chronic Inflammatory Demyelinating PolyradiculoneuropathyDocument5 pagesChronic Inflammatory Demyelinating PolyradiculoneuropathyDiego Fernando AlegriaPas encore d'évaluation
- The Administration of Medications I. Speaking 'Administering Medications'Document5 pagesThe Administration of Medications I. Speaking 'Administering Medications'Meri AndaniPas encore d'évaluation
- Measuring Central Venous Pressure: Elaine ColeDocument8 pagesMeasuring Central Venous Pressure: Elaine ColednllkzaPas encore d'évaluation
- KSPCB BIOMEDICAL POSTER 1aDocument1 pageKSPCB BIOMEDICAL POSTER 1armulmadgiPas encore d'évaluation
- Glaser, R., & Kiecolt-Glaser, J. K. (2005) - Stress-Induced Immune DysfunctionDocument9 pagesGlaser, R., & Kiecolt-Glaser, J. K. (2005) - Stress-Induced Immune DysfunctionFranco Paolo Maray-GhigliottoPas encore d'évaluation
- Gastroenterology Evaluation TemplateDocument2 pagesGastroenterology Evaluation Templatee-MedTools88% (8)
- Lista Preturi Teste Genetice GendiaDocument227 pagesLista Preturi Teste Genetice GendiaMatei FloriPas encore d'évaluation
- Allergic Contact DermatitisDocument12 pagesAllergic Contact DermatitisAzis BoenjaminPas encore d'évaluation
- Feeling GreatDocument243 pagesFeeling GreatSunny LamPas encore d'évaluation
- Tolak Angin TranslatedDocument3 pagesTolak Angin TranslatedWadz MuharPas encore d'évaluation
- Worksheet 4, Ubaidillah, 3BDocument6 pagesWorksheet 4, Ubaidillah, 3BUbay SegaPas encore d'évaluation
- SupradynDocument5 pagesSupradynashrayagrawalPas encore d'évaluation
- Festival Dance Lesson - Module 2 - P.E. 3rd Quarter PPT 2 of 2Document29 pagesFestival Dance Lesson - Module 2 - P.E. 3rd Quarter PPT 2 of 2Maria Fe VibarPas encore d'évaluation
- Acute Gastritis CiciDocument43 pagesAcute Gastritis CiciDwi Rezky AmaliaPas encore d'évaluation
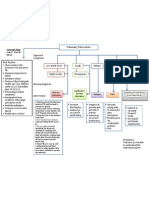
- Concept Map PTBDocument1 pageConcept Map PTBJoan Abardo100% (2)
- Anesthesia For The Pet Practitioner (Banfield, 2003 Edition) PDFDocument125 pagesAnesthesia For The Pet Practitioner (Banfield, 2003 Edition) PDFKatarina SimicicPas encore d'évaluation
- NCPDocument2 pagesNCPfierfizPas encore d'évaluation
- Case Study of Most Common Communicable DiseasesDocument13 pagesCase Study of Most Common Communicable DiseasesnesjynPas encore d'évaluation
- PRE Test 1Document15 pagesPRE Test 1Naomi VirtudazoPas encore d'évaluation
- SP42 Thoracentesis (Adult)Document7 pagesSP42 Thoracentesis (Adult)Adam HuzaibyPas encore d'évaluation
- @MBS MedicalBooksStore 2020 CompressionDocument46 pages@MBS MedicalBooksStore 2020 CompressionTaufikPas encore d'évaluation
- Counseling TechniquesDocument60 pagesCounseling Techniquesdinalen0% (1)
- Behavioral Health Care Plan: Assessment DataDocument9 pagesBehavioral Health Care Plan: Assessment Dataapi-521018364Pas encore d'évaluation
- Needle Prick Injury & PreventionDocument17 pagesNeedle Prick Injury & Preventioniman zainuddinPas encore d'évaluation
- Vertical Root Fracture !Document42 pagesVertical Root Fracture !Dr Dithy kkPas encore d'évaluation
- CH 14 Antepartum Nursing Assessment NotesDocument8 pagesCH 14 Antepartum Nursing Assessment NotesMary LowryPas encore d'évaluation
- Meningococcal Infection in ChildrenDocument6 pagesMeningococcal Infection in ChildrenAdrian KhomanPas encore d'évaluation
- Shah - Cancer of The Head and Neck PDFDocument12 pagesShah - Cancer of The Head and Neck PDFElizabetha SalzcenPas encore d'évaluation
- HOẰNG HÓA 4-THANH HÓA 2022Document6 pagesHOẰNG HÓA 4-THANH HÓA 2022Tuấn KhanhPas encore d'évaluation