Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- 2016 Emergency and Trauma Radiology - A Teaching File Opt VXDocument415 pages2016 Emergency and Trauma Radiology - A Teaching File Opt VXRe S100% (5)
- Institute of Neurosciences Kolkata (Schedule) PDFDocument2 pagesInstitute of Neurosciences Kolkata (Schedule) PDFpvkdasaPas encore d'évaluation
- Maternal & Child Nursing Bullets (Nle & Nclex)Document38 pagesMaternal & Child Nursing Bullets (Nle & Nclex)Richard Ines Valino95% (22)
- The Term Aplastic Anemia Indicates: Pancytopenia in The PresenceDocument34 pagesThe Term Aplastic Anemia Indicates: Pancytopenia in The PresenceKhadar mohamedPas encore d'évaluation
- Start CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorDocument2 pagesStart CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorFelicia ErikaPas encore d'évaluation
- Benign Prostatic Hyperplasia Concept MapDocument1 pageBenign Prostatic Hyperplasia Concept MapSarah RonquilloPas encore d'évaluation
- Causes of Erectile Dysfunction As Explained in AyurvedaDocument25 pagesCauses of Erectile Dysfunction As Explained in Ayurvedacharanmann9165Pas encore d'évaluation
- Common Bile Duct Stones StrictureDocument48 pagesCommon Bile Duct Stones StrictureSyarif MalawatPas encore d'évaluation
- Gestational Trophoblastic Disease (Neha Martin Msc. NSG 2nd Year)Document13 pagesGestational Trophoblastic Disease (Neha Martin Msc. NSG 2nd Year)Gunu SinghPas encore d'évaluation
- Sistema Curativo Por Dieta Amucosa - Arnold Ehret - WWW - Arnoldehret.infoDocument8 pagesSistema Curativo Por Dieta Amucosa - Arnold Ehret - WWW - Arnoldehret.infoLorena CalahorroPas encore d'évaluation
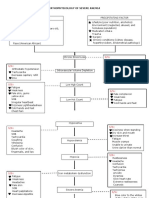
- Pathophysiology of Severe AnemiaDocument3 pagesPathophysiology of Severe AnemiaChrizley Shawn DeroniaPas encore d'évaluation
- Xeljanz Initiation ChecklistDocument8 pagesXeljanz Initiation ChecklistRawan ZayedPas encore d'évaluation
- Ayurvedic Nail Analysis: What Do Your Nails Say About Your HealthDocument14 pagesAyurvedic Nail Analysis: What Do Your Nails Say About Your Healthsirrichard1Pas encore d'évaluation
- Difference Between Signs and SymptomsDocument5 pagesDifference Between Signs and SymptomsSitlalin RamosPas encore d'évaluation
- NSAIDS in CKDDocument12 pagesNSAIDS in CKDDanni XPas encore d'évaluation
- عبد الرحمن خالد الزميلي Assighment Of Dental Surgery /Principle of routine exodontiaDocument20 pagesعبد الرحمن خالد الزميلي Assighment Of Dental Surgery /Principle of routine exodontiaعبد الرحمن خالد الزميليPas encore d'évaluation
- History and Objectives of Post Marketing SurveillanceDocument14 pagesHistory and Objectives of Post Marketing SurveillanceSohit Gupta100% (1)
- Cystic FibrosisDocument4 pagesCystic Fibrosisapi-548375486Pas encore d'évaluation
- Headache When To WorryDocument9 pagesHeadache When To Worryezra_putriPas encore d'évaluation
- Soft Tissue SarcomaDocument19 pagesSoft Tissue SarcomaEkvanDanangPas encore d'évaluation
- Drug Study 2Document8 pagesDrug Study 2rey_tengPas encore d'évaluation
- Seyfert 2009Document6 pagesSeyfert 2009yane sofPas encore d'évaluation
- Ketoconazole Cream Clinical ParticularsDocument2 pagesKetoconazole Cream Clinical ParticularsJai MurugeshPas encore d'évaluation
- Common Symptoms of Gastrointestinal and Abdominal DiseaseDocument34 pagesCommon Symptoms of Gastrointestinal and Abdominal DiseaseMalueth AnguiPas encore d'évaluation
- Holstein B Cell Lecture 11-13-14Document47 pagesHolstein B Cell Lecture 11-13-14Alex DennisPas encore d'évaluation
- Mcqs of Endocrine SystemDocument25 pagesMcqs of Endocrine SystemkajuPas encore d'évaluation
- DRUG STUDY (Mefenamic Acid)Document4 pagesDRUG STUDY (Mefenamic Acid)Paolo Digo67% (6)
- Dipiros Pharmacotherapy Handbook 12Th Edition Terry L Schwinghammer Full ChapterDocument67 pagesDipiros Pharmacotherapy Handbook 12Th Edition Terry L Schwinghammer Full Chapterian.costa277100% (13)
- 3rd Year Nursing MS LEC MIDTERM QUIZESDocument18 pages3rd Year Nursing MS LEC MIDTERM QUIZESAudrie Allyson GabalesPas encore d'évaluation
- The Amyloid Beta Peptide A Chemist S Perspective. Role in Alzheimer's and FibrillizationDocument46 pagesThe Amyloid Beta Peptide A Chemist S Perspective. Role in Alzheimer's and FibrillizationAdrianEPas encore d'évaluation