Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Borders Crossed: Vibhishana in The Ramayana and Beyond: South Asia: Journal of South Asian StudiesDocument22 pagesBorders Crossed: Vibhishana in The Ramayana and Beyond: South Asia: Journal of South Asian StudieskarmayagnaPas encore d'évaluation
- Spiritual Development Through The Chakra Progression: Jennifer Drapkin, Clayton Mcclintock, Elsa Lau, Lisa MillerDocument16 pagesSpiritual Development Through The Chakra Progression: Jennifer Drapkin, Clayton Mcclintock, Elsa Lau, Lisa MillerkarmayagnaPas encore d'évaluation
- Flowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupsDocument1 pageFlowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupskarmayagnaPas encore d'évaluation
- Flow Chart of The Manufacturing Process Used by Arena Software Numbers Indicating BatchDocument1 pageFlow Chart of The Manufacturing Process Used by Arena Software Numbers Indicating BatchkarmayagnaPas encore d'évaluation
- Manufacturing Process MapDocument1 pageManufacturing Process MapkarmayagnaPas encore d'évaluation
- Logical Flow Diagram of The Production Process OperationsDocument1 pageLogical Flow Diagram of The Production Process OperationskarmayagnaPas encore d'évaluation
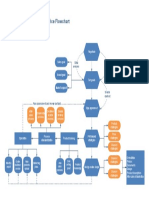
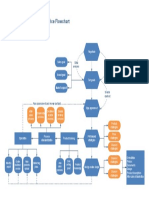
- Ecommerce FlowchartDocument1 pageEcommerce FlowchartkarmayagnaPas encore d'évaluation
- BhagavadGita theArtofLeadership OldTextNewContextDocument19 pagesBhagavadGita theArtofLeadership OldTextNewContextkarmayagnaPas encore d'évaluation
- Manufacturing WorkflowDocument1 pageManufacturing WorkflowDidik HariadiPas encore d'évaluation
- Logical Flow Diagram of The Production Process OperationsDocument1 pageLogical Flow Diagram of The Production Process OperationskarmayagnaPas encore d'évaluation
- Main Functions of The Operative Manufacturing Execution LevelDocument1 pageMain Functions of The Operative Manufacturing Execution LevelkarmayagnaPas encore d'évaluation
- Manufacturing Process MapDocument1 pageManufacturing Process MapkarmayagnaPas encore d'évaluation
- Beer Processing PFDDocument1 pageBeer Processing PFDkarmayagnaPas encore d'évaluation
- Flowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupsDocument1 pageFlowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupskarmayagnaPas encore d'évaluation
- Order WorkflowDocument1 pageOrder WorkflowkarmayagnaPas encore d'évaluation
- Logical Flow Diagram of The Production Process OperationsDocument1 pageLogical Flow Diagram of The Production Process OperationskarmayagnaPas encore d'évaluation
- Manufacturing WorkflowDocument1 pageManufacturing WorkflowDidik HariadiPas encore d'évaluation
- Beer Production ProcessDocument1 pageBeer Production ProcesskarmayagnaPas encore d'évaluation
- Server WorkflowDocument1 pageServer WorkflowkarmayagnaPas encore d'évaluation
- Order FlowchartDocument1 pageOrder FlowchartkarmayagnaPas encore d'évaluation
- Intra Arterial ChemotherapyDocument6 pagesIntra Arterial ChemotherapykarmayagnaPas encore d'évaluation
- Services FlowchartDocument1 pageServices FlowchartLuis Fernando Sanchez TapiaPas encore d'évaluation
- Survival After Oral CancerDocument5 pagesSurvival After Oral CancerkarmayagnaPas encore d'évaluation
- Quality Control Process: Material SupplierDocument1 pageQuality Control Process: Material Supplieralva10 vaPas encore d'évaluation
- Statistical Study For Sonographic Differential Diagnosis ofDocument8 pagesStatistical Study For Sonographic Differential Diagnosis ofkarmayagnaPas encore d'évaluation
- Outcome of SQ .Cell CA of GingivaDocument5 pagesOutcome of SQ .Cell CA of GingivakarmayagnaPas encore d'évaluation
- Ecommerce FlowchartDocument1 pageEcommerce FlowchartkarmayagnaPas encore d'évaluation
- Oral CancerDocument5 pagesOral CancerkarmayagnaPas encore d'évaluation
- Secondary Orbital MlanomasDocument5 pagesSecondary Orbital MlanomaskarmayagnaPas encore d'évaluation
- Vision Guided Precision CultivationDocument18 pagesVision Guided Precision CultivationAndré QuirinoPas encore d'évaluation
- Earnings Management Using Classification Shifting: An Examination of Core Earnings and Special ItemsDocument31 pagesEarnings Management Using Classification Shifting: An Examination of Core Earnings and Special ItemsFridRachmanPas encore d'évaluation
- SFM SiddharthDocument17 pagesSFM SiddharthSiddharth SangtaniPas encore d'évaluation
- Statgraphics Plus: Alphabetical List of Analyses and FeaturesDocument19 pagesStatgraphics Plus: Alphabetical List of Analyses and FeaturesjosePas encore d'évaluation
- Quartiles Deciles and PercentilesDocument9 pagesQuartiles Deciles and PercentilesClerenda Mcgrady100% (1)
- Improving Global Seismic Event Locations Using Source-Receiver ReciprocityDocument10 pagesImproving Global Seismic Event Locations Using Source-Receiver Reciprocitymanuelflorez1102Pas encore d'évaluation
- Dan Shuster's Exploring Data AP StatisticsDocument3 pagesDan Shuster's Exploring Data AP Statisticsgoogle0987Pas encore d'évaluation
- Statistical Quality Control in LaboratoryDocument11 pagesStatistical Quality Control in Laboratoryabhijit612100% (1)
- Math As A ToolDocument31 pagesMath As A ToolDasha LopezPas encore d'évaluation
- 02-BCA-Statistical Methods and Their ApplicationsDocument1 page02-BCA-Statistical Methods and Their ApplicationsKrishna Chaitanya BramheswaramPas encore d'évaluation
- Segunda Asignación de Estadística Aplicada A La Ingeniería Química 2017 IIDocument4 pagesSegunda Asignación de Estadística Aplicada A La Ingeniería Química 2017 IIAnonymous u7Z8KWXPas encore d'évaluation
- Clinical Retention Force Development of Double CrownsDocument6 pagesClinical Retention Force Development of Double CrownsVero AngelPas encore d'évaluation
- Quantitative Mathematics Module 1 PDFDocument8 pagesQuantitative Mathematics Module 1 PDFyelzPas encore d'évaluation
- 10.1.1.136.1024-Performance in Noise and InterferenceDocument110 pages10.1.1.136.1024-Performance in Noise and InterferenceRomualdo Begale PrudêncioPas encore d'évaluation
- Industrial Engineering & Enterprise Resource Planning: Statistical Quality ControlDocument41 pagesIndustrial Engineering & Enterprise Resource Planning: Statistical Quality ControlVaibhav Vithoba Naik100% (1)
- Zhang Et Al. (2016)Document43 pagesZhang Et Al. (2016)prempatilPas encore d'évaluation
- MCQ 2Document4 pagesMCQ 2Prakash SinghPas encore d'évaluation
- University of Cambridge International Examinations General Certificate of Education Advanced Subsidiary Level and Advanced LevelDocument4 pagesUniversity of Cambridge International Examinations General Certificate of Education Advanced Subsidiary Level and Advanced LevelHubbak KhanPas encore d'évaluation
- Biostatistics Word NewDocument43 pagesBiostatistics Word NewMereesha K MoideenPas encore d'évaluation
- Ncert Solutions For Class 11 Maths May22 Chapter 15 StatisticsDocument52 pagesNcert Solutions For Class 11 Maths May22 Chapter 15 StatisticsPriyanshuPas encore d'évaluation
- Astm e 2262 - 03Document48 pagesAstm e 2262 - 03Francisco GuerraPas encore d'évaluation
- Quartile For Ungroup DataDocument37 pagesQuartile For Ungroup DataallenkingPas encore d'évaluation
- Ms-08 Comlete Book - Unit - 9Document305 pagesMs-08 Comlete Book - Unit - 9anandjaymishra0% (1)
- Mid Term Exam StatBusiness 2019-2020 Set F PDFDocument13 pagesMid Term Exam StatBusiness 2019-2020 Set F PDFJon SnowPas encore d'évaluation
- Math SymbolsDocument11 pagesMath SymbolsRussell MurphyPas encore d'évaluation
- Btac 492Document9 pagesBtac 492lbqurtftsPas encore d'évaluation
- Kothari 2005 - Performance Matched DiscretionaryDocument35 pagesKothari 2005 - Performance Matched DiscretionaryBerliana Anggun DewintaPas encore d'évaluation
- Publishable FormatDocument9 pagesPublishable FormatRon Santelices100% (1)
- Measuring Cost Risk of Buildings and Building Systems: Standard Practice ForDocument9 pagesMeasuring Cost Risk of Buildings and Building Systems: Standard Practice ForAhmad Zubair RasulyPas encore d'évaluation