Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Obstetric FormDocument4 pagesObstetric FormKhylamarie VillalunaPas encore d'évaluation
- DR Paul Krawitz - Ultimate Insiders Guide To Eye HealthDocument60 pagesDR Paul Krawitz - Ultimate Insiders Guide To Eye HealthPro APas encore d'évaluation
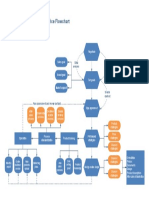
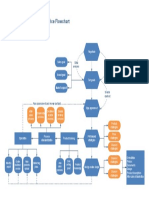
- Ecommerce FlowchartDocument1 pageEcommerce FlowchartkarmayagnaPas encore d'évaluation
- Advanced EndodonticsDocument375 pagesAdvanced EndodonticsSaleh Alsadi100% (1)
- General Paper September 2020Document26 pagesGeneral Paper September 2020Kumah Wisdom100% (1)
- Borders Crossed: Vibhishana in The Ramayana and Beyond: South Asia: Journal of South Asian StudiesDocument22 pagesBorders Crossed: Vibhishana in The Ramayana and Beyond: South Asia: Journal of South Asian StudieskarmayagnaPas encore d'évaluation
- Manufacturing Process MapDocument1 pageManufacturing Process MapkarmayagnaPas encore d'évaluation
- BhagavadGita theArtofLeadership OldTextNewContextDocument19 pagesBhagavadGita theArtofLeadership OldTextNewContextkarmayagnaPas encore d'évaluation
- Manufacturing WorkflowDocument1 pageManufacturing WorkflowDidik HariadiPas encore d'évaluation
- Spiritual Development Through The Chakra Progression: Jennifer Drapkin, Clayton Mcclintock, Elsa Lau, Lisa MillerDocument16 pagesSpiritual Development Through The Chakra Progression: Jennifer Drapkin, Clayton Mcclintock, Elsa Lau, Lisa MillerkarmayagnaPas encore d'évaluation
- Flowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupsDocument1 pageFlowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupskarmayagnaPas encore d'évaluation
- Main Functions of The Operative Manufacturing Execution LevelDocument1 pageMain Functions of The Operative Manufacturing Execution LevelkarmayagnaPas encore d'évaluation
- Logical Flow Diagram of The Production Process OperationsDocument1 pageLogical Flow Diagram of The Production Process OperationskarmayagnaPas encore d'évaluation
- Flow Chart of The Manufacturing Process Used by Arena Software Numbers Indicating BatchDocument1 pageFlow Chart of The Manufacturing Process Used by Arena Software Numbers Indicating BatchkarmayagnaPas encore d'évaluation
- Manufacturing Process MapDocument1 pageManufacturing Process MapkarmayagnaPas encore d'évaluation
- Statistical Study For Sonographic Differential Diagnosis ofDocument8 pagesStatistical Study For Sonographic Differential Diagnosis ofkarmayagnaPas encore d'évaluation
- Flowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupsDocument1 pageFlowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupskarmayagnaPas encore d'évaluation
- Logical Flow Diagram of The Production Process OperationsDocument1 pageLogical Flow Diagram of The Production Process OperationskarmayagnaPas encore d'évaluation
- Services FlowchartDocument1 pageServices FlowchartLuis Fernando Sanchez TapiaPas encore d'évaluation
- Beer Production ProcessDocument1 pageBeer Production ProcesskarmayagnaPas encore d'évaluation
- Beer Processing PFDDocument1 pageBeer Processing PFDkarmayagnaPas encore d'évaluation
- Server WorkflowDocument1 pageServer WorkflowkarmayagnaPas encore d'évaluation
- Manufacturing WorkflowDocument1 pageManufacturing WorkflowDidik HariadiPas encore d'évaluation
- Order WorkflowDocument1 pageOrder WorkflowkarmayagnaPas encore d'évaluation
- Quality Control Process: Material SupplierDocument1 pageQuality Control Process: Material Supplieralva10 vaPas encore d'évaluation
- Ecommerce FlowchartDocument1 pageEcommerce FlowchartkarmayagnaPas encore d'évaluation
- Order FlowchartDocument1 pageOrder FlowchartkarmayagnaPas encore d'évaluation
- Logical Flow Diagram of The Production Process OperationsDocument1 pageLogical Flow Diagram of The Production Process OperationskarmayagnaPas encore d'évaluation
- Survival After Oral CancerDocument5 pagesSurvival After Oral CancerkarmayagnaPas encore d'évaluation
- Oral CancerDocument5 pagesOral CancerkarmayagnaPas encore d'évaluation
- Secondary Orbital MlanomasDocument5 pagesSecondary Orbital MlanomaskarmayagnaPas encore d'évaluation
- Outcome of SQ .Cell CA of GingivaDocument5 pagesOutcome of SQ .Cell CA of GingivakarmayagnaPas encore d'évaluation
- Relationship of Tumor Thickness in Punch Biopsy and SubsequentDocument4 pagesRelationship of Tumor Thickness in Punch Biopsy and SubsequentkarmayagnaPas encore d'évaluation
- SalesDocument1 pageSalesapi-77587316Pas encore d'évaluation
- 295 QsDocument3 pages295 Qsujangketul62Pas encore d'évaluation
- Clinical Case Studies 2013 Bunaciu 179 98Document21 pagesClinical Case Studies 2013 Bunaciu 179 98adri90Pas encore d'évaluation
- Branding Strategies DecisionsDocument40 pagesBranding Strategies DecisionsnishatalicoolPas encore d'évaluation
- Aetiology of Canine Infectious Respiratory Disease Complex and Prevalence of Its Pathogens in EuropeDocument23 pagesAetiology of Canine Infectious Respiratory Disease Complex and Prevalence of Its Pathogens in EuropeNadia AbarcaPas encore d'évaluation
- (Ped-W1) (Dr. Zuhair M. Al Musawi) Repiratory 2Document43 pages(Ped-W1) (Dr. Zuhair M. Al Musawi) Repiratory 2Haider Nadhem AL-rubaiPas encore d'évaluation
- Republic Act No. 6675: Reporter: Manamparan Hosny MDocument17 pagesRepublic Act No. 6675: Reporter: Manamparan Hosny Mkhara teanoPas encore d'évaluation
- FamilyDocument19 pagesFamilytugba1234Pas encore d'évaluation
- Annual Report 2010Document72 pagesAnnual Report 2010Yan-Lin Jubi LeePas encore d'évaluation
- Overt Diabetes in PregnancyDocument12 pagesOvert Diabetes in PregnancyGestne AurePas encore d'évaluation
- Drug Study Folic AcidDocument2 pagesDrug Study Folic Acid6fq2cmfgn4Pas encore d'évaluation
- Minnesota Fall School Planning Guide - Minnesota Department of HealthDocument16 pagesMinnesota Fall School Planning Guide - Minnesota Department of HealthPatch Minnesota100% (1)
- Postural, DrainageDocument7 pagesPostural, DrainageJames ThompsonPas encore d'évaluation
- Head TraumaDocument4 pagesHead TraumaDinarkram Rabreca EculPas encore d'évaluation
- PedoDocument2 pagesPedoHenyo AkoPas encore d'évaluation
- Handwashing BoothDocument8 pagesHandwashing Boothapi-284180001Pas encore d'évaluation
- Characterization of Renal Stones Using Gsi: Patient HistoryDocument2 pagesCharacterization of Renal Stones Using Gsi: Patient HistoryAlreem AlhajryPas encore d'évaluation
- Frankenstein Application EssayDocument6 pagesFrankenstein Application Essaymyra Thiong'oPas encore d'évaluation
- Hand Hygiene Audit March 19Document17 pagesHand Hygiene Audit March 19Sammie WainainaPas encore d'évaluation
- SgotsgptDocument23 pagesSgotsgptUmi MazidahPas encore d'évaluation
- Presented by Amir Sadaula BVSC & Ah, 8 Sem Rampur Campus Roll No: 01Document19 pagesPresented by Amir Sadaula BVSC & Ah, 8 Sem Rampur Campus Roll No: 01naturalamirPas encore d'évaluation
- Drug Name Mechanism of Action Dosage/ Route Indication/ Contraindication Side Effects/ Adverse Reaction Nursing ResponsibilitiesDocument1 pageDrug Name Mechanism of Action Dosage/ Route Indication/ Contraindication Side Effects/ Adverse Reaction Nursing ResponsibilitiesLowell AgustinPas encore d'évaluation
- Nausea and VomitingDocument6 pagesNausea and VomitingRavinderPas encore d'évaluation
- Iir 2013 14Document347 pagesIir 2013 14SHESH RAJPRABHAKARPas encore d'évaluation
- Eating Disorders: by Pius KigamwaDocument20 pagesEating Disorders: by Pius KigamwaRahul Kumar DiwakarPas encore d'évaluation
- Life Insurance Corporation of India Novel Coronavirus (Covid-19) Questionnaire (Revised Version - 5)Document1 pageLife Insurance Corporation of India Novel Coronavirus (Covid-19) Questionnaire (Revised Version - 5)பிரேம் முருகன்Pas encore d'évaluation