Vous aimerez peut-être aussi
- Liver Function Tests (LFTS) : Git Block 1 Lecture Dr. Usman GhaniDocument26 pagesLiver Function Tests (LFTS) : Git Block 1 Lecture Dr. Usman Ghaniraanja2100% (1)
- Liver FunctionDocument90 pagesLiver Functionapi-19641337Pas encore d'évaluation
- Immunomodulation in Domestic Food Animals: Advances in Veterinary Science and Comparative MedicineD'EverandImmunomodulation in Domestic Food Animals: Advances in Veterinary Science and Comparative MedicineBernald CharleyPas encore d'évaluation
- Preview PDFDocument117 pagesPreview PDFbernardo100% (1)
- Liver function tests: Van den Bergh test and assessment of secretory functionDocument7 pagesLiver function tests: Van den Bergh test and assessment of secretory functionadiPas encore d'évaluation
- Characteristics of Hemostasis During Experimental Ehrlichia Canis InfectionDocument9 pagesCharacteristics of Hemostasis During Experimental Ehrlichia Canis InfectionDiana Granada100% (1)
- 62 Lecture Menstrual Cycle Abnormalities, Infertility, MenopauseDocument69 pages62 Lecture Menstrual Cycle Abnormalities, Infertility, MenopauseTarek TarekPas encore d'évaluation
- Clinical Biochemistry - Clinical Pathology and Procedures - VetDocument9 pagesClinical Biochemistry - Clinical Pathology and Procedures - VetHimmet AslanPas encore d'évaluation
- Trace ElementsDocument5 pagesTrace ElementsFaithPas encore d'évaluation
- Constipation Risk Assessment ToolDocument2 pagesConstipation Risk Assessment ToolAnggie Anggriyana100% (1)
- Oestrogen, Progesterone, AndrogensDocument58 pagesOestrogen, Progesterone, AndrogensTandin SonamPas encore d'évaluation
- Acid Base Balance OR OR Regulation of Blood PHDocument175 pagesAcid Base Balance OR OR Regulation of Blood PHhirendra patel100% (1)
- Liver Function Testing PDFDocument2 pagesLiver Function Testing PDFRajesh KumarPas encore d'évaluation
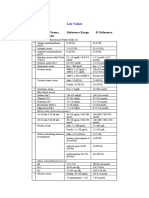
- Blood, Plasma, Serum Reference Range SI Reference: Lab ValuesDocument4 pagesBlood, Plasma, Serum Reference Range SI Reference: Lab ValuesEvaG2012Pas encore d'évaluation
- Equine Gastric Ulcers / A Presentation by Wendy Harless Mollat, DVM, DACVIM, Pilchuck Veterinary HospitalDocument47 pagesEquine Gastric Ulcers / A Presentation by Wendy Harless Mollat, DVM, DACVIM, Pilchuck Veterinary HospitalPilchuck Veterinary HospitalPas encore d'évaluation
- RINJUDocument35 pagesRINJUதீபன்குமார் கதிரேசன்100% (1)
- G6PD, GalactosemiaDocument32 pagesG6PD, GalactosemiaEricka B. BanaszczukPas encore d'évaluation
- Fluid and Electrolyte Balance: Compartments of Body and Distribution of Water by WeightDocument137 pagesFluid and Electrolyte Balance: Compartments of Body and Distribution of Water by Weight0921pyPas encore d'évaluation
- Problem Based Learning Case Study Thyroid DisorderDocument30 pagesProblem Based Learning Case Study Thyroid DisorderdrnawafPas encore d'évaluation
- Git 2Document18 pagesGit 2Mateen ShukriPas encore d'évaluation
- Animal Models in Experimental Gastric Ulcer Screening-A ReviewDocument6 pagesAnimal Models in Experimental Gastric Ulcer Screening-A Reviewnareshph28Pas encore d'évaluation
- Inborn Errors of Metabolism - Basics For Students (Iver Andreas Norbergs Kopi Som Er I Konflikt 2016-01-24)Document4 pagesInborn Errors of Metabolism - Basics For Students (Iver Andreas Norbergs Kopi Som Er I Konflikt 2016-01-24)Wen Jie LauPas encore d'évaluation
- Case Study 2Document12 pagesCase Study 2api-336539272Pas encore d'évaluation
- Renal Lab Tests ExplainedDocument67 pagesRenal Lab Tests ExplainedRjDPas encore d'évaluation
- Compensatory Mechanism of Circulatory ShockDocument29 pagesCompensatory Mechanism of Circulatory ShockWan Razin Wan Hassan100% (1)
- Biliary DyskinesiaDocument1 pageBiliary DyskinesiaYolotl Hilario Sanchez CarrilloPas encore d'évaluation
- Celiac DiseaseDocument53 pagesCeliac DiseaseAndrew FongPas encore d'évaluation
- Electrolyte and Metabolic Panel GuideDocument24 pagesElectrolyte and Metabolic Panel GuideDanish KamalPas encore d'évaluation
- Diabetes Investigation & Management GuideDocument36 pagesDiabetes Investigation & Management GuideBHEEMREDDY VIVEKREDDY100% (1)
- Mind Map: Amino Acid MetabolismDocument1 pageMind Map: Amino Acid MetabolismAbbey Ayala100% (1)
- Biochemical Tests Dietary IntakeDocument10 pagesBiochemical Tests Dietary IntakeDawlat SalamaPas encore d'évaluation
- Worst Kept Secrets - Toxic Inert Ingredients in Pesticides - NCAPDocument15 pagesWorst Kept Secrets - Toxic Inert Ingredients in Pesticides - NCAPaxyzaaa100% (1)
- Urine AnalysisDocument53 pagesUrine AnalysisMaath KhalidPas encore d'évaluation
- Swu Phinma, College of Pharmacy 2020: Wr/Urinalysis - Html#Ixzz6Zxlj RQKH /Product-Manual/3008 - 3B - UrinalysisDocument7 pagesSwu Phinma, College of Pharmacy 2020: Wr/Urinalysis - Html#Ixzz6Zxlj RQKH /Product-Manual/3008 - 3B - UrinalysisTrex MarciiiPas encore d'évaluation
- Lecture 28 - Pathology of DiabetesDocument34 pagesLecture 28 - Pathology of Diabetesapi-3703352100% (4)
- BLOOD PresentationDocument33 pagesBLOOD PresentationLezlie Jane SahaliPas encore d'évaluation
- UNIT: Total and Direct BilirubinDocument10 pagesUNIT: Total and Direct BilirubinbiddyusmcPas encore d'évaluation
- Pharmacotherapeutics, Pharmacodynamics & Pharmacokinetics ExplainedDocument47 pagesPharmacotherapeutics, Pharmacodynamics & Pharmacokinetics ExplainedAshaPas encore d'évaluation
- 3.dietary Surveillance and Nutritional Assessment in England PDFDocument25 pages3.dietary Surveillance and Nutritional Assessment in England PDFAbdul RazakPas encore d'évaluation
- Interpret Liver TestsDocument4 pagesInterpret Liver TestsKaram Ali ShahPas encore d'évaluation
- Liver Dysfunction: Clinical BiochemistryDocument45 pagesLiver Dysfunction: Clinical BiochemistryLitha Mega PrastikaPas encore d'évaluation
- What Is The Oral Glucose Tolerance TestDocument2 pagesWhat Is The Oral Glucose Tolerance TestBianca Camille100% (1)
- AnemiaDocument41 pagesAnemiaBang FadPas encore d'évaluation
- Injuria Renal Aguda PDFDocument7 pagesInjuria Renal Aguda PDFCaaarolPas encore d'évaluation
- Allergy and HypersensitivityDocument73 pagesAllergy and HypersensitivityAdi PomeranzPas encore d'évaluation
- Lab 9++10 Pathological UrinlysisDocument38 pagesLab 9++10 Pathological UrinlysisSai SreedharPas encore d'évaluation
- FUNCTIONALFOODSDocument93 pagesFUNCTIONALFOODSNicoleta RotaruPas encore d'évaluation
- Diagnosis of Feline Infectious Peritonitis (FIP)Document2 pagesDiagnosis of Feline Infectious Peritonitis (FIP)lecol351100% (1)
- Vitamin B12 Deficiency and A Patient Case StudyDocument36 pagesVitamin B12 Deficiency and A Patient Case Studynherm6425100% (1)
- Clinical Signs in Humans and Animals Associated with Minerals, Trace Elements and Rare Earth ElementsD'EverandClinical Signs in Humans and Animals Associated with Minerals, Trace Elements and Rare Earth ElementsPas encore d'évaluation
- Infectious Diseases of The Dog and Cat, A Color Handbook (VetBooks - Ir)Document329 pagesInfectious Diseases of The Dog and Cat, A Color Handbook (VetBooks - Ir)alrsxvxPas encore d'évaluation
- Medication Use in Older Adults by Rose Knapp, MSN, RN, APRN-BC, ANPDocument34 pagesMedication Use in Older Adults by Rose Knapp, MSN, RN, APRN-BC, ANPJose Antonio Tous OlagortaPas encore d'évaluation
- Fact File Gastro Intestinal HormonesDocument2 pagesFact File Gastro Intestinal HormonesSudip DevadasPas encore d'évaluation
- Effects of Hormones On Metabolic RateDocument6 pagesEffects of Hormones On Metabolic RatemjfphotoPas encore d'évaluation
- Biochemical MethodDocument35 pagesBiochemical MethodKrizzel Almazora100% (1)
- Determination of PKa Values For APIDocument9 pagesDetermination of PKa Values For APISimona Florina Precup100% (1)
- Questions Renal Physiology Find The Mode of Action of A Diuretic DrugDocument3 pagesQuestions Renal Physiology Find The Mode of Action of A Diuretic DrugGroup A1G30% (1)
- Gastrointestinal Diseases and Disorders Sourcebook, Fifth EditionD'EverandGastrointestinal Diseases and Disorders Sourcebook, Fifth EditionPas encore d'évaluation
- The Leukotrienes: Chemistry and BiologyD'EverandThe Leukotrienes: Chemistry and BiologyLawrence ChakrinPas encore d'évaluation
- Internal Vet. Med. Exam April 2010Document3 pagesInternal Vet. Med. Exam April 2010Ali H. Sadiek أ.د. علي حسن صديقPas encore d'évaluation
- Follow Up Exam April 2009Document12 pagesFollow Up Exam April 2009Ali H. Sadiek أ.د. علي حسن صديق100% (1)
- Follow Up Exam April 2009Document12 pagesFollow Up Exam April 2009Ali H. Sadiek أ.د. علي حسن صديق100% (1)
- Azoturia, Paralytic Myoglobinuria of EquineDocument16 pagesAzoturia, Paralytic Myoglobinuria of EquineAli H. Sadiek أ.د. علي حسن صديق100% (1)
- Water and Electrolyte Homeostasis For Vet. StudentsDocument45 pagesWater and Electrolyte Homeostasis For Vet. StudentsAli H. Sadiek أ.د. علي حسن صديق100% (2)
- Final Term Exam For 5th Year Student (Internal Vet. Med. Part II.Document3 pagesFinal Term Exam For 5th Year Student (Internal Vet. Med. Part II.Ali H. Sadiek أ.د. علي حسن صديق100% (1)
- Acid Base Disorders For Vet. StudentsDocument43 pagesAcid Base Disorders For Vet. StudentsAli H. Sadiek أ.د. علي حسن صديق100% (2)
- Rhinitis in Domestic AnimalsDocument15 pagesRhinitis in Domestic AnimalsAli H. Sadiek أ.د. علي حسن صديق100% (2)
- ELISA in Comparison With Conventional Methods For Detection ofDocument9 pagesELISA in Comparison With Conventional Methods For Detection ofAli H. Sadiek أ.د. علي حسن صديق100% (1)
- Metabolic Diseases, Milk Fever by Ali SadiekDocument30 pagesMetabolic Diseases, Milk Fever by Ali SadiekAli H. Sadiek أ.د. علي حسن صديق100% (3)
- Post Parturient HemoglobinuriaDocument12 pagesPost Parturient HemoglobinuriaAli H. Sadiek أ.د. علي حسن صديق67% (3)
- Buffalo Health and Disease For AVSSADocument51 pagesBuffalo Health and Disease For AVSSAAli H. Sadiek أ.د. علي حسن صديق100% (5)
- Postparturient Hypomagnesemia, Grass TetanyDocument21 pagesPostparturient Hypomagnesemia, Grass TetanyAli H. Sadiek أ.د. علي حسن صديق50% (2)
- Downer Cow Syndrome, Creeper Cows.Document8 pagesDowner Cow Syndrome, Creeper Cows.Ali H. Sadiek أ.د. علي حسن صديق100% (1)
- Role of Cryptosporidial Infection F. Osman and Ali SadiekDocument10 pagesRole of Cryptosporidial Infection F. Osman and Ali SadiekAli H. Sadiek أ.د. علي حسن صديق100% (4)
- Respiratory System Disease RSDDocument19 pagesRespiratory System Disease RSDAli H. Sadiek أ.د. علي حسن صديق100% (1)
- Simple Indigestion in RuminantsDocument11 pagesSimple Indigestion in RuminantsAli H. Sadiek أ.د. علي حسن صديق75% (4)
- Vagus Indigestionعسر الهضم المسبب باصابة العصب الحائرDocument27 pagesVagus Indigestionعسر الهضم المسبب باصابة العصب الحائرAli H. Sadiek أ.د. علي حسن صديق100% (3)
- Gastritis, Gastric Ulcer and Gastric Rupture in Monogastric Animals by Ali SadiekDocument27 pagesGastritis, Gastric Ulcer and Gastric Rupture in Monogastric Animals by Ali SadiekAli H. Sadiek أ.د. علي حسن صديق100% (6)
- Gastric Dilatation in Monogastric Animals by Ali SadiekDocument8 pagesGastric Dilatation in Monogastric Animals by Ali SadiekAli H. Sadiek أ.د. علي حسن صديقPas encore d'évaluation
- Omasoabomasal Impaction in A Gersy CowDocument6 pagesOmasoabomasal Impaction in A Gersy CowAli H. Sadiek أ.د. علي حسن صديق100% (1)
- Peritonitis in farm animals by Ali Sadiek الالتهاب البريتوني في حيوانات المزرعةDocument27 pagesPeritonitis in farm animals by Ali Sadiek الالتهاب البريتوني في حيوانات المزرعةAli H. Sadiek أ.د. علي حسن صديق100% (2)
- Hepatic Problems in Farm Animal by Prof. Ali SadiekDocument23 pagesHepatic Problems in Farm Animal by Prof. Ali SadiekAli H. Sadiek أ.د. علي حسن صديقPas encore d'évaluation
- Diseases of The Intestine of Farm Animals by Ali Sadiek Vet. Med. AssiutDocument47 pagesDiseases of The Intestine of Farm Animals by Ali Sadiek Vet. Med. AssiutAli H. Sadiek أ.د. علي حسن صديق100% (9)
- Diseases of Pahyrinx and Esophagus in Farm Animals by Ali SadiekDocument39 pagesDiseases of Pahyrinx and Esophagus in Farm Animals by Ali SadiekAli H. Sadiek أ.د. علي حسن صديق100% (4)
- Diseases of Nervous System of Farm Animals by Ali SadiekDocument65 pagesDiseases of Nervous System of Farm Animals by Ali SadiekAli H. Sadiek أ.د. علي حسن صديق100% (7)
- Traumatic Reticuloperitonitis by Ali SadiekDocument32 pagesTraumatic Reticuloperitonitis by Ali SadiekAli H. Sadiek أ.د. علي حسن صديق100% (7)
- Ruminal Acidosis/Rumen Overload For Vet. Students /ali SadiekDocument25 pagesRuminal Acidosis/Rumen Overload For Vet. Students /ali SadiekAli H. Sadiek أ.د. علي حسن صديق100% (2)
- Diseases of The Abomasum For Vet. Student by Ali SadiekDocument36 pagesDiseases of The Abomasum For Vet. Student by Ali SadiekAli H. Sadiek أ.د. علي حسن صديق100% (1)
- Tympany in Ruminants by Ali Sadiek Assiut Univ.Document27 pagesTympany in Ruminants by Ali Sadiek Assiut Univ.Ali H. Sadiek أ.د. علي حسن صديق100% (9)
- 6-Liver Function TestsDocument5 pages6-Liver Function TestsAhmed ImranPas encore d'évaluation
- Bagan KolestasisDocument1 pageBagan KolestasisSoma SkaPas encore d'évaluation
- Interpretation of Liver Function TestsDocument14 pagesInterpretation of Liver Function TestsNirav SharmaPas encore d'évaluation
- Neonatal JaundiceDocument33 pagesNeonatal JaundiceVaibhav Krishna100% (2)
- Clinical Case On JaundiceDocument43 pagesClinical Case On JaundicePro fatherPas encore d'évaluation
- Liver FunctionDocument24 pagesLiver FunctionramireddyPas encore d'évaluation
- Daftar Pustaka Skripsi Daun CiplukanDocument4 pagesDaftar Pustaka Skripsi Daun CiplukanshonsakarisaPas encore d'évaluation
- CholecystitisDocument10 pagesCholecystitisKamilatun NiamahPas encore d'évaluation
- Date Year Hs Code Product QuantityunitDocument45 pagesDate Year Hs Code Product QuantityunitProschool HyderabadPas encore d'évaluation
- VIDocument5 pagesVIRaymark Sabanal Gaudia0% (1)
- Deuxieme MagasinDocument5 pagesDeuxieme MagasinYacouba DembelePas encore d'évaluation
- Clinical Chem II FactsheetsDocument46 pagesClinical Chem II FactsheetsmeriiPas encore d'évaluation
- Drug Induced Liver DiseaseDocument15 pagesDrug Induced Liver DiseaseMUGHALPas encore d'évaluation
- LFT LalpathDocument2 pagesLFT Lalpathmoyic39272Pas encore d'évaluation
- NCM 118a Lec 9 Liver FailureDocument9 pagesNCM 118a Lec 9 Liver FailureJan Crizza Dale R. FrancoPas encore d'évaluation
- Abdominal UltrasoundDocument6 pagesAbdominal Ultrasounds0800841739100% (1)
- Acute CholecystitisDocument3 pagesAcute CholecystitisًPas encore d'évaluation
- CholelithiasisDocument6 pagesCholelithiasisLara GatbontonPas encore d'évaluation
- Chronic Hepatitis BDocument5 pagesChronic Hepatitis BMurat HessesPas encore d'évaluation
- JaundiceDocument3 pagesJaundiceNyaoNyao MarcellanaPas encore d'évaluation
- IcterusDocument11 pagesIcterusnikita134Pas encore d'évaluation
- Jurnal IkterusDocument3 pagesJurnal IkterusTututWidyaNurAnggrainiPas encore d'évaluation
- Fatty Liver Signs & Symptoms ExplainedDocument3 pagesFatty Liver Signs & Symptoms ExplainedIshika KohliPas encore d'évaluation
- Doziranje antipiretika u djeceDocument1 pageDoziranje antipiretika u djeceNatalija BokanPas encore d'évaluation
- Hepatitis: Jump To Navigation Jump To SearchDocument11 pagesHepatitis: Jump To Navigation Jump To SearchZely ApriantiPas encore d'évaluation
- Liver Tumors BasicDocument37 pagesLiver Tumors BasicSahirPas encore d'évaluation
- Liver Function Tests: Presented By-Dr. Arshiya Kaura (JR 1)Document50 pagesLiver Function Tests: Presented By-Dr. Arshiya Kaura (JR 1)vikasPas encore d'évaluation
- 3 Konsep Terapi ARVDocument65 pages3 Konsep Terapi ARVkristinaPas encore d'évaluation
- EASL Clinical Practice Guidelines: Autoimmune HepatitisDocument34 pagesEASL Clinical Practice Guidelines: Autoimmune HepatitisBety Puma PauccaraPas encore d'évaluation
- FibroscanDocument3 pagesFibroscanAri WirantariPas encore d'évaluation