Vous aimerez peut-être aussi
- Expresspay Revision FormDocument1 pageExpresspay Revision Formapi-114425407Pas encore d'évaluation
- Erie EFT PDFDocument2 pagesErie EFT PDFAnonymous rNfN6DiaPas encore d'évaluation
- EFT Form - Fillable - LifeDocument2 pagesEFT Form - Fillable - LifeZachPas encore d'évaluation
- Primary Account Holder Joint Account Holder 1 Joint Account Holder 2Document1 pagePrimary Account Holder Joint Account Holder 1 Joint Account Holder 2Varun NagpalPas encore d'évaluation
- Bank Authorization (BA) FormDocument4 pagesBank Authorization (BA) FormAilec FinancesPas encore d'évaluation
- EPCORPaymentPlanApplication EdmontonFortisDocument3 pagesEPCORPaymentPlanApplication EdmontonFortiskevinatstarburstPas encore d'évaluation
- BUCKS CONCRETE & PAVERS INC - AmTrust Workers' Compensation PolicyDocument37 pagesBUCKS CONCRETE & PAVERS INC - AmTrust Workers' Compensation PolicyYvette BroadwaterPas encore d'évaluation
- Truist Ach FormDocument1 pageTruist Ach FormhugstinsPas encore d'évaluation
- Standing Instruction Form Through IndusInd Bank Account-2Document1 pageStanding Instruction Form Through IndusInd Bank Account-2SonuPas encore d'évaluation
- Electronic Payment (EP) Account Agreement: Things To Know Before You BeginDocument4 pagesElectronic Payment (EP) Account Agreement: Things To Know Before You BeginandryPas encore d'évaluation
- Universal Member Application: Personal InformationDocument2 pagesUniversal Member Application: Personal InformationHunter GrayPas encore d'évaluation
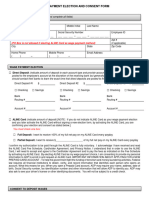
- Adp Wage Payment Election and Consent FormDocument2 pagesAdp Wage Payment Election and Consent FormjermarionPas encore d'évaluation
- Uib 1091aDocument2 pagesUib 1091aJoseph SantosPas encore d'évaluation
- Care Credit AppDocument7 pagesCare Credit AppwvhvetPas encore d'évaluation
- ABSLIC - NACH, ECS, Auto Direct Debit FormDocument2 pagesABSLIC - NACH, ECS, Auto Direct Debit FormBHARAT PRAKASH MAHANT0% (2)
- Credit Repair Plan B Expedite Agreement 05-13-16Document9 pagesCredit Repair Plan B Expedite Agreement 05-13-16Plan B CRSPas encore d'évaluation
- Dir DepDocument1 pageDir Depfazlah8106Pas encore d'évaluation
- Non Federal Direct Deposit Enrollment Request Form EnglishDocument1 pageNon Federal Direct Deposit Enrollment Request Form EnglishtobyPas encore d'évaluation
- Pionex Institution Due Diligence List-Word VerDocument3 pagesPionex Institution Due Diligence List-Word Versalmanhameed42Pas encore d'évaluation
- Form 0000000290Document1 pageForm 0000000290Deacon Wm Spencer Powell Sr.Pas encore d'évaluation
- TenantenrollDocument1 pageTenantenrollapi-243721603Pas encore d'évaluation
- FedLoanServicing - Direct DepositDocument2 pagesFedLoanServicing - Direct DepositEric Li Cheungtastic100% (1)
- Credit Card Automatic Payment Plan (Autopay) : 1. Customer DetailsDocument4 pagesCredit Card Automatic Payment Plan (Autopay) : 1. Customer DetailsaksynPas encore d'évaluation
- OM UnitTrust DO AmendmentForm (FINAL) ElectronicDocument6 pagesOM UnitTrust DO AmendmentForm (FINAL) ElectronicMonika ShanikaPas encore d'évaluation
- Renewal Ecs Latest Form - 8.9.2017Document1 pageRenewal Ecs Latest Form - 8.9.2017Priya SelvarajPas encore d'évaluation
- Partial Withdrawal FormDocument2 pagesPartial Withdrawal FormPinkys Venkat100% (1)
- FOR Office USE Only: HDFC Life Sb/Ca/Cc/Sb-Nre/Sb-Nro/OtherDocument2 pagesFOR Office USE Only: HDFC Life Sb/Ca/Cc/Sb-Nre/Sb-Nro/OtherVIkashPas encore d'évaluation
- LONG Validation LetterDocument3 pagesLONG Validation LetterJim Work100% (1)
- Direct Deposit Enrollment & Changes: SECTION 1: Annuitant InformationDocument3 pagesDirect Deposit Enrollment & Changes: SECTION 1: Annuitant InformationdesireePas encore d'évaluation
- Mandate For ECS ADI NWDocument1 pageMandate For ECS ADI NWRipal PatelPas encore d'évaluation
- Generic Form Preview DocumentDocument1 pageGeneric Form Preview Documentelena.69.mxPas encore d'évaluation
- Special Instructions:: Check-O-Matic AuthorizationDocument2 pagesSpecial Instructions:: Check-O-Matic AuthorizationMinh HuynhPas encore d'évaluation
- Direct Deposit FormDocument3 pagesDirect Deposit FormSreenivas RaoPas encore d'évaluation
- Forms Payout Others Web 23 AprilDocument2 pagesForms Payout Others Web 23 AprilYo PaisaPas encore d'évaluation
- Application and Credit Card Account Agreement: 1. APPLICANT INFORMATION: Please Tell Us About YourselfDocument8 pagesApplication and Credit Card Account Agreement: 1. APPLICANT INFORMATION: Please Tell Us About Yourselfsaxmachine1411Pas encore d'évaluation
- 197 - Excess Contribution and Deposit Correcti..Document1 page197 - Excess Contribution and Deposit Correcti..tdrkPas encore d'évaluation
- NACH FormDocument1 pageNACH FormPrem Singh Mehta75% (4)
- FOR Office USE Only: HDFC Life Sb/Ca/Cc/Sb-Nre/Sb-Nro/OtherDocument2 pagesFOR Office USE Only: HDFC Life Sb/Ca/Cc/Sb-Nre/Sb-Nro/OtherAnithaPas encore d'évaluation
- Policy Surrender Form PDFDocument2 pagesPolicy Surrender Form PDF1012804201Pas encore d'évaluation
- Registration Form Cum Mandate For Electronic Clearing Services (Ecs) /direct Debit/NachDocument2 pagesRegistration Form Cum Mandate For Electronic Clearing Services (Ecs) /direct Debit/NachPatel DipenPas encore d'évaluation
- Printapplication GE SSDocument8 pagesPrintapplication GE SSmgworkPas encore d'évaluation
- NACH ModifiedDocument1 pageNACH ModifiederbgawdwePas encore d'évaluation
- Direct Deposit FormDocument3 pagesDirect Deposit FormRabindra ShakyaPas encore d'évaluation
- Sbi New Ecs FormDocument1 pageSbi New Ecs FormzampakPas encore d'évaluation
- Disposal Instruction For Handling Foreign Inward RemittancesDocument3 pagesDisposal Instruction For Handling Foreign Inward RemittancesSelvamuthu KumaranPas encore d'évaluation
- F 9465Document3 pagesF 9465Pat PlantePas encore d'évaluation
- Borrower Declaration - CA & LEI RegulationDocument2 pagesBorrower Declaration - CA & LEI RegulationSHASHI KANTPas encore d'évaluation
- Sheila McCorriston WithdrawalDocument14 pagesSheila McCorriston WithdrawalAnonymous BmFjIMShq9100% (1)
- Security Bank ADA Enrollment FormDocument1 pageSecurity Bank ADA Enrollment FormNoknik OllirecPas encore d'évaluation
- Installment Payment AgreementDocument1 pageInstallment Payment AgreementAct Pornlapus100% (1)
- Payout RequestDocument2 pagesPayout RequestInfopedia OnlineherePas encore d'évaluation
- New Credit AppDocument5 pagesNew Credit Appapi-282795606Pas encore d'évaluation
- Pre Auth FormDocument2 pagesPre Auth FormemaanazeemPas encore d'évaluation
- Direct Debit Form 200010-2259-A4Document2 pagesDirect Debit Form 200010-2259-A4bluffboy55Pas encore d'évaluation
- Credit Repair KitDocument9 pagesCredit Repair KitChristine Skiba0% (1)
- Registration Form Cum Mandate For Electronic Clearing Services (Ecs) /direct Debit/NachDocument2 pagesRegistration Form Cum Mandate For Electronic Clearing Services (Ecs) /direct Debit/NachG.R.AzhaguvelSaranya Professor MechanicalPas encore d'évaluation
- Caoile EFT Authorization Form - EnglishDocument2 pagesCaoile EFT Authorization Form - EnglishSaki DacaraPas encore d'évaluation
- Wiltby Final-Final DraftDocument10 pagesWiltby Final-Final Draftapi-114425407Pas encore d'évaluation
- Portfolio EssayDocument9 pagesPortfolio Essayapi-114425407Pas encore d'évaluation
- Wiltby Final-Final DraftDocument10 pagesWiltby Final-Final Draftapi-114425407Pas encore d'évaluation
- Commercial Driver QuestionnaireDocument2 pagesCommercial Driver Questionnaireapi-114425407Pas encore d'évaluation
- Personal Driver QuestionnaireDocument2 pagesPersonal Driver Questionnaireapi-114425407Pas encore d'évaluation