Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Evaluation of Microscopic HematuriaDocument15 pagesEvaluation of Microscopic HematuriaAndi SusiloPas encore d'évaluation
- Types of JaundiceDocument3 pagesTypes of Jaundicesintia mariaPas encore d'évaluation
- Sjögren's Syndrome. A Case Study - MFHDocument3 pagesSjögren's Syndrome. A Case Study - MFHManuel Flores HernandezPas encore d'évaluation
- Cancer of LarynxDocument29 pagesCancer of LarynxQasim HaleimiPas encore d'évaluation
- CDC E. Coli FactsheetDocument2 pagesCDC E. Coli Factsheetbutter-mmPas encore d'évaluation
- Typhoid Fever: Presented by Sharlin MacalintalDocument18 pagesTyphoid Fever: Presented by Sharlin MacalintalPaul JacksonPas encore d'évaluation
- Nursing Care PlanDocument3 pagesNursing Care PlanJASMINE JOY BADUAPas encore d'évaluation
- Information On Diabetes Explicit Misery Are Expected To Work On The Nature of Diabetes CareDocument2 pagesInformation On Diabetes Explicit Misery Are Expected To Work On The Nature of Diabetes CareBashar Al-AhmadPas encore d'évaluation
- Incursions Learning Objectives/Study Guide: EEDA/IAT Web-Based CourseDocument7 pagesIncursions Learning Objectives/Study Guide: EEDA/IAT Web-Based Coursevdcastillo13Pas encore d'évaluation
- Internal Medicine II II MidtermDocument11 pagesInternal Medicine II II MidtermJerin XavierPas encore d'évaluation
- Amoebiasis in Wild Mammals: Ayesha Ahmed M Phil. Parasitology 1 Semester 2013-Ag-2712Document25 pagesAmoebiasis in Wild Mammals: Ayesha Ahmed M Phil. Parasitology 1 Semester 2013-Ag-2712Abdullah AzeemPas encore d'évaluation
- Internatinal 1Document5 pagesInternatinal 1daffunkmadansyahPas encore d'évaluation
- Health Declaration Form (Annex A2) - KoronadalDocument3 pagesHealth Declaration Form (Annex A2) - KoronadalJephte MantalabaPas encore d'évaluation
- 29-09-2020 HMB EnglishDocument22 pages29-09-2020 HMB EnglishNeeraj S GPas encore d'évaluation
- AUH Travel Declaration FormDocument2 pagesAUH Travel Declaration FormAbdul RahmanPas encore d'évaluation
- Acromegaly Feb2020Document4 pagesAcromegaly Feb2020anlekgenPas encore d'évaluation
- Nursing Care Plan: St. Anthony's College San Jose, Antique Nursing Department NameDocument2 pagesNursing Care Plan: St. Anthony's College San Jose, Antique Nursing Department NameKristine Young100% (1)
- Key Health Indicators Basic Information: State Health Profile - Madhya PradeshDocument2 pagesKey Health Indicators Basic Information: State Health Profile - Madhya PradeshvinayrhtPas encore d'évaluation
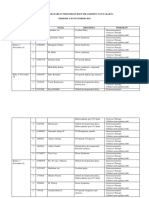
- Logbook Harian Fisioterapi Rsup DR SardjitoDocument9 pagesLogbook Harian Fisioterapi Rsup DR SardjitoAnindya YusriaPas encore d'évaluation
- Role of The Nurse in Stroke RehabilitationDocument2 pagesRole of The Nurse in Stroke RehabilitationAnonymous mTqyS6Pas encore d'évaluation
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormJudeLaxPas encore d'évaluation
- Surgery III MCQS 2023Document4 pagesSurgery III MCQS 2023mariamPas encore d'évaluation
- Framingham Heart Study PDFDocument5 pagesFramingham Heart Study PDFCarlos Fernando RíosPas encore d'évaluation
- CuesDocument8 pagesCuesFloyd SevillaPas encore d'évaluation
- Khorana AA - Thromboembolism in Hospitalized Neutropenic Cancer PatientsDocument8 pagesKhorana AA - Thromboembolism in Hospitalized Neutropenic Cancer PatientsFarid RakhmanPas encore d'évaluation
- Summary Chart of U.S. Medical Eligibility Criteria For Contraceptive UseDocument2 pagesSummary Chart of U.S. Medical Eligibility Criteria For Contraceptive UseBlessy AbrahamPas encore d'évaluation
- BIU Clinic FormsDocument4 pagesBIU Clinic FormsMarvellous AbrahamPas encore d'évaluation
- Anaerobic Bacteria QuizletDocument6 pagesAnaerobic Bacteria QuizletReca Marie FRIASPas encore d'évaluation
- COC Exam 2019 For HO (1) - 250321095434Document66 pagesCOC Exam 2019 For HO (1) - 250321095434Behar Abduraheman83% (6)
- Lana Moussa Aleech - Senior Project Research PaperDocument13 pagesLana Moussa Aleech - Senior Project Research Paperapi-655770614Pas encore d'évaluation