Vous aimerez peut-être aussi
- PPT-"Services and Benefits For Gulf War Veterans" - Anthony HardieDocument98 pagesPPT-"Services and Benefits For Gulf War Veterans" - Anthony HardieAnthony Hardie100% (5)
- AGAINST COVID Vaccines: Follow Protocol C For at Least 21 Days + Protocol K at The Place of The InjectionDocument11 pagesAGAINST COVID Vaccines: Follow Protocol C For at Least 21 Days + Protocol K at The Place of The Injectionearl-e-birdPas encore d'évaluation
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsD'EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsÉvaluation : 5 sur 5 étoiles5/5 (9)
- Nursing Care of CHF (Congestive Heart Failure)Document25 pagesNursing Care of CHF (Congestive Heart Failure)Irwan100% (2)
- VACCINATION DANGERS - The Health Hazards of Disease Prevention - BSEM-2011Document45 pagesVACCINATION DANGERS - The Health Hazards of Disease Prevention - BSEM-2011bigbill138Pas encore d'évaluation
- Lucija Tomljenovic - The Vaccination Policy and The Code of Practice of The JCVIDocument45 pagesLucija Tomljenovic - The Vaccination Policy and The Code of Practice of The JCVITratincica StewartPas encore d'évaluation
- Pediatrics 2012 780 92Document15 pagesPediatrics 2012 780 92ERICKPas encore d'évaluation
- SHEA-APIC Guideline - Infection Prevention and Control in The Long-Term Care FacilityDocument53 pagesSHEA-APIC Guideline - Infection Prevention and Control in The Long-Term Care FacilityAqsha RamadhanisaPas encore d'évaluation
- Dietician Referral Ms SmithDocument3 pagesDietician Referral Ms SmithPrasoon Premraj0% (1)
- Urine Culture: D.M.M. LabDocument15 pagesUrine Culture: D.M.M. LabTomi RahmadaniPas encore d'évaluation
- Immunization Programs For Infants, Children, Adolescents, and Adults: Clinical Practice Guidelines by The Infectious Diseases Society of AmericaDocument24 pagesImmunization Programs For Infants, Children, Adolescents, and Adults: Clinical Practice Guidelines by The Infectious Diseases Society of AmericaEugene YeboahPas encore d'évaluation
- Vacunas 2012Document7 pagesVacunas 2012dr.alexisleon9124Pas encore d'évaluation
- States, 2011 United Recommended Childhood and Adolescent Immunization SchedulesDocument7 pagesStates, 2011 United Recommended Childhood and Adolescent Immunization SchedulesDolores KilpatrickPas encore d'évaluation
- MMWR HiB PDFDocument20 pagesMMWR HiB PDFworksheetbookPas encore d'évaluation
- Adult ScheduleDocument3 pagesAdult ScheduledrmanojvimalPas encore d'évaluation
- Adult Immunization ScheduleDocument3 pagesAdult Immunization Schedulemo0nseerratPas encore d'évaluation
- General Best PracticeDocument193 pagesGeneral Best PracticegrigmihPas encore d'évaluation
- Vaccines - The Week in Review - 3 January 2011Document16 pagesVaccines - The Week in Review - 3 January 2011davidrcurryPas encore d'évaluation
- Retraction-Ileal-lymphoid-nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenDocument1 pageRetraction-Ileal-lymphoid-nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenOutlawHealthPas encore d'évaluation
- 2019 Guide For ImmunizationDocument195 pages2019 Guide For ImmunizationReigner paul DavidPas encore d'évaluation
- Adult Immunization ScheduleDocument3 pagesAdult Immunization ScheduleBryan Mae H. DegorioPas encore d'évaluation
- CHN 1 LEC WEEK 9 Records in Family Health Nursing PracticeDocument14 pagesCHN 1 LEC WEEK 9 Records in Family Health Nursing PracticeSenyorita ArdiPas encore d'évaluation
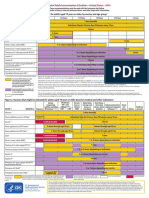
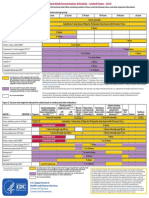
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDocument2 pagesFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasPas encore d'évaluation
- Annotated BibliographyDocument12 pagesAnnotated BibliographyJOSEPHPas encore d'évaluation
- Adult Combined ScheduleDocument5 pagesAdult Combined SchedulelcmurilloPas encore d'évaluation
- Adult Pocafeket SizeDocument2 pagesAdult Pocafeket SizedadfPas encore d'évaluation
- Inequalities in Full Immunization Coverage: Trends in Low-And Middle - Income CountriesDocument13 pagesInequalities in Full Immunization Coverage: Trends in Low-And Middle - Income CountrieshasanPas encore d'évaluation
- Prevention Control of InfluenzaDocument60 pagesPrevention Control of Influenzajamesgarrow100% (2)
- z30tq Pediatric Nutrition Handbook 6th EditionDocument52 pagesz30tq Pediatric Nutrition Handbook 6th EditionJair OsorioPas encore d'évaluation
- Policy BriefDocument10 pagesPolicy Briefapi-438364488Pas encore d'évaluation
- Hepatitis B Vaccination Coverage Among Health-Care Personnel in The United StatesDocument12 pagesHepatitis B Vaccination Coverage Among Health-Care Personnel in The United StatesRio MulyaPas encore d'évaluation
- Jur Geru New 1Document7 pagesJur Geru New 1redyhataPas encore d'évaluation
- The Value of Vaccination A Global PerspeDocument13 pagesThe Value of Vaccination A Global Perspethedevilsoul981Pas encore d'évaluation
- InfuenzaDocument30 pagesInfuenzaChandra_INHU_RiauPas encore d'évaluation
- Reading VaccineImmunizationDocument13 pagesReading VaccineImmunizationelztly4694Pas encore d'évaluation
- Right To Refuse Flu ShotsDocument4 pagesRight To Refuse Flu ShotsBZ Riger100% (2)
- Hepatitis Vaccines: Keywords: Hepatitis A, B, C, D, and E VaccinesDocument18 pagesHepatitis Vaccines: Keywords: Hepatitis A, B, C, D, and E VaccinesPutri Anita AchmadPas encore d'évaluation
- NAC Hospi UCI y SalasDocument10 pagesNAC Hospi UCI y Salasgiseladelarosa2006Pas encore d'évaluation
- Pediatrics 2000 Johnson 1006 12Document9 pagesPediatrics 2000 Johnson 1006 12Amelia ArnisPas encore d'évaluation
- Rotavirus Vaccine and Health Care Utilization For Diarrhea in U.S. ChildrenDocument10 pagesRotavirus Vaccine and Health Care Utilization For Diarrhea in U.S. ChildrenErlangga Perwira NegaraPas encore d'évaluation
- Immunization in The United States: Recommendations, Barriers, and Measures To Improve ComplianceDocument2 pagesImmunization in The United States: Recommendations, Barriers, and Measures To Improve CompliancecaaarleeyPas encore d'évaluation
- Monitoring of Patients On Long-Term Glucocorticoid TherapyDocument10 pagesMonitoring of Patients On Long-Term Glucocorticoid TherapyFitriyana WinarnoPas encore d'évaluation
- Research Paper On Childhood VaccinationsDocument8 pagesResearch Paper On Childhood Vaccinationsefjr9yx3100% (1)
- Clinical Practice Guideline For The Evaluation of Fever and Infection in Older Adult Residents of Long-Term Care Facilities - 2008 Update by The Infectious Diseases Society of AmericaDocument23 pagesClinical Practice Guideline For The Evaluation of Fever and Infection in Older Adult Residents of Long-Term Care Facilities - 2008 Update by The Infectious Diseases Society of AmericaReyner LeonPas encore d'évaluation
- Extent of Compliance To Immunization Reasons For Non Continuity and Its Consequences PDFDocument26 pagesExtent of Compliance To Immunization Reasons For Non Continuity and Its Consequences PDFAPRIL LYNPas encore d'évaluation
- Department of Health and Human Services: Office of The SecretaryDocument10 pagesDepartment of Health and Human Services: Office of The SecretaryAnonymous QDbBPZhwqGPas encore d'évaluation
- Data Update: A Summary of Global Immunization Coverage Through 2011Document5 pagesData Update: A Summary of Global Immunization Coverage Through 2011dwbrown_6Pas encore d'évaluation
- Vacunación de Profesionales de La SaludDocument48 pagesVacunación de Profesionales de La SaludfcarcamoPas encore d'évaluation
- Guia IDSA Prevencion ICVCDocument32 pagesGuia IDSA Prevencion ICVCmaturana61Pas encore d'évaluation
- Coronavirus Vaccine - Summary of Yellow Card Reporting: Data Included: 09/12/2020 To 07/03/2021Document17 pagesCoronavirus Vaccine - Summary of Yellow Card Reporting: Data Included: 09/12/2020 To 07/03/2021José BacigalupoPas encore d'évaluation
- IDSAasdsfDocument46 pagesIDSAasdsfAnonymous d3qpXcm4xVPas encore d'évaluation
- RRL VaccineDocument6 pagesRRL VaccineAlexandra Mae D. MiguelPas encore d'évaluation
- 10 1016@j Vaccine 2017 10 011 PDFDocument10 pages10 1016@j Vaccine 2017 10 011 PDFAmare AlemuPas encore d'évaluation
- Comment: For Lancet On Universal Universal-Health-CoverageDocument2 pagesComment: For Lancet On Universal Universal-Health-Coverageapi-112905159Pas encore d'évaluation
- Pneumonii 2007Document46 pagesPneumonii 2007Turcu AndreeaPas encore d'évaluation
- Influenza Vaccination: Healthcare Workers Attitude in Three Middle East CountriesDocument7 pagesInfluenza Vaccination: Healthcare Workers Attitude in Three Middle East CountriesDesti EryaniPas encore d'évaluation
- Expanded Program On ImmunizationDocument6 pagesExpanded Program On ImmunizationAiza Oronce100% (1)
- 2006 118 1774-1793 Subcommittee On Diagnosis and Management of BronchiolitisDocument22 pages2006 118 1774-1793 Subcommittee On Diagnosis and Management of BronchiolitisAlejandra Castro Salas エールPas encore d'évaluation
- Essential Medicines at The National Level: The Global Asthma Network's Essential Asthma Medicines Survey 2014Document15 pagesEssential Medicines at The National Level: The Global Asthma Network's Essential Asthma Medicines Survey 2014erzenkrasniqiPas encore d'évaluation
- Adult Combined ScheduleDocument5 pagesAdult Combined ScheduleAwal Safar MPas encore d'évaluation
- English 101 Final EssayDocument13 pagesEnglish 101 Final EssayHa HangPas encore d'évaluation
- 2016 Article 3107Document8 pages2016 Article 3107Alvaro LugoPas encore d'évaluation
- Influenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?D'EverandInfluenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?Pas encore d'évaluation
- The Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionD'EverandThe Vaccine Handbook: A Practical Guide for Clinicians, Twelfth EditionPas encore d'évaluation
- Critical Hits Rolls by Josef Tham, v2.0 atDocument3 pagesCritical Hits Rolls by Josef Tham, v2.0 atghostvalleyPas encore d'évaluation
- Maternal Obesity and Diabetes Mellitus As Risk Factors For Congenital Heart Disease in The OffspringDocument9 pagesMaternal Obesity and Diabetes Mellitus As Risk Factors For Congenital Heart Disease in The OffspringBianca CaterinalisendraPas encore d'évaluation
- March 2012Document28 pagesMarch 2012Bill5199Pas encore d'évaluation
- Polysomnography (PSG) : Patient Information Patient InformationDocument12 pagesPolysomnography (PSG) : Patient Information Patient Informationhotland sitorusPas encore d'évaluation
- Pacemakers - Fact SheetDocument7 pagesPacemakers - Fact Sheettalha.k.rajpootPas encore d'évaluation
- 014 Nursing (GNM) III Final RevaluationDocument1 page014 Nursing (GNM) III Final Revaluationhr7.bccnPas encore d'évaluation
- Gastrointestinal Diseases During Pregnancy What DoDocument11 pagesGastrointestinal Diseases During Pregnancy What Dotakechi takechiPas encore d'évaluation
- Urnal Vox Sanguinis - 2023 - Pons - Prevalence of Red Blood Cell Alloantibodies Among Blood Donors in The French Military BloodDocument5 pagesUrnal Vox Sanguinis - 2023 - Pons - Prevalence of Red Blood Cell Alloantibodies Among Blood Donors in The French Military BloodFauzan.APas encore d'évaluation
- Contact Nummular (Discoid) Eczema From Depilating Cream: Case ReportDocument2 pagesContact Nummular (Discoid) Eczema From Depilating Cream: Case ReportMorindaPas encore d'évaluation
- Therapeutic Plasma Exchange in Thrombotic Thrombocytopenic PurpuraDocument9 pagesTherapeutic Plasma Exchange in Thrombotic Thrombocytopenic Purpurasugi9namliPas encore d'évaluation
- Emergency Viva (Full)Document48 pagesEmergency Viva (Full)ashokarathnasinghePas encore d'évaluation
- POT Lesson PlanDocument4 pagesPOT Lesson PlanMichelle TheresePas encore d'évaluation
- By: Abduljabbar Hamid Jabbar: University of Baghdad-College of Medicine M. B. Ch. BDocument14 pagesBy: Abduljabbar Hamid Jabbar: University of Baghdad-College of Medicine M. B. Ch. BXena XenaPas encore d'évaluation
- Case Report Large Uterine Fibroids in Pregnancy With Successful Caesarean MyomectomyDocument4 pagesCase Report Large Uterine Fibroids in Pregnancy With Successful Caesarean MyomectomyChidimma VictoryPas encore d'évaluation
- Vandana Raut Tata Memorial Centre 31yrsDocument2 pagesVandana Raut Tata Memorial Centre 31yrsvandanaPas encore d'évaluation
- Product CatalogDocument32 pagesProduct Catalogharshad koyandePas encore d'évaluation
- I. General Physical AssessmentDocument5 pagesI. General Physical AssessmentmnlstrPas encore d'évaluation
- FC Derm (SA) Regulations 26-3-2014Document13 pagesFC Derm (SA) Regulations 26-3-2014matentenPas encore d'évaluation
- 5 - DOWNLOAD Lactobacillus Acidophilus Rosell 52Document6 pages5 - DOWNLOAD Lactobacillus Acidophilus Rosell 52everstrongPas encore d'évaluation
- Literature Review Ectopic PregnancyDocument4 pagesLiterature Review Ectopic Pregnancyakjnbowgf100% (1)
- EMPANELEDHOSPITALLISTDocument12 pagesEMPANELEDHOSPITALLISTVsknPas encore d'évaluation
- Abortion in CattleDocument6 pagesAbortion in CattlekumarpujariPas encore d'évaluation
- Endocrine PancreasDocument21 pagesEndocrine Pancreaslacafey741Pas encore d'évaluation
- Failure of Weaning:: According To The European Respiratory Society (ERS) Task ForceDocument12 pagesFailure of Weaning:: According To The European Respiratory Society (ERS) Task ForceAmr El Taher0% (1)
- Formularium 2017Document87 pagesFormularium 2017Venita AgustinaPas encore d'évaluation