Académique Documents
Professionnel Documents
Culture Documents
Super Final Output (For Hardbound)
Transféré par
Melody Kaye MonsantoDescription originale:
Titre original
Copyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
Super Final Output (For Hardbound)
Transféré par
Melody Kaye MonsantoDroits d'auteur :
Formats disponibles
CHAPTER 1 THE PROBLEM
Introduction Infection with the Human Immunodeficiency Virus (HIV) results in destruction of the bodys host defenses and immune system leading to the condition called Acquired Immune Deficiency
Syndrome (AIDS). HIV-AIDS is one of the worlds greatest public health crises. For many years, because of lack of understanding and effective treatment, it is now considered a rapidly progressing fatal disease. HIV infection in humans is considered pandemic by the World Health Organization (WHO). The Center for Disease Control and Prevention (2003) reported that there are more than 20 million died from HIV-AIDS globally. The Department of Health National Epidemiology Center (2011) reported that from 1984 to 2011, there were 860 AIDS cases reported, 71 percent (613) were males. Of the reported AIDS cases, 323 (38 percent) had already died at the time of case reporting. Sexual contact was the most common mode of HIV transmission, accounting for 93 percent (799) of all reported AIDS cases. The
number of HIV cases continues its upward trend, with the latest figure in January 2011, there were 152 new HIV Ab sero-positive individuals confirmed by the STD/AIDS Cooperative Central
Laboratory (SACCL) and reported to the HIV and AIDS Registry. This was a 6 percent increase compared to the same period last year. Most of the cases (93 percent) were males. In the Philippines, HIV is recently considered to be epidemic. This means that Filipinos should not remain passive, instead, be aware of the nature of transmission of this fast spreading deadly disease. In this study, the researchers are focusing on the level of awareness in one of the high-risk groups the out-of-school youth. According to Dr. Jerie P. Calingasan, Cagayan de Oro City Health Officer, there are 31 reported cases of HIV-AIDS throughout the city, as of December, 2011. He exclaimed that there is really a need for the promotion of HIV-AIDS awareness not only to specific groups but to everyone. According to the Department of Education, Camaman-an National High School ranked 15th among all the 35 public secondary schools in Cagayan de Oro City in terms of highest drop rate which is 5.53 percent in the school year 2009-2010. In 2011, the drop rate increased to 7.77 percent which shove them to the 9th rank. Aside
from being a part of Xavier University community, Barangay Camaman-an was chosen in terms of its total population, which has a larger number compared to the others which ranked higher than Camaman-an. It is through these reasons that the researchers desire to know the level of awareness of this vulnerable group of our society the out-of-school youth about HIV-AIDS. The fact that they are not in school; they might be deprived of knowledge about sexual and reproductive health, unless they are informed by their parents, friends or media. Conceptual Framework This study is based on the following concepts: As defined in Websters Comprehensive Dictionary, Level of awareness is the degree of knowledge or consciousness. In this study, it refers to the extent of the awareness of the out of school youth regarding HIV-AIDS. It is categorized as highly, moderately, fairly aware or unaware. In the study of Laguna (2004) on Knowledge of HIV/AIDS and Unsafe Sex Practices among Filipino Youth, it is believed that increasing the awareness on the realities of HIV/AIDS, can modify behaviors, specifically, risky sexual practices. There is an almost
universal awareness of AIDS among young people ages 15-24. Ninety five percent said they have heard of AIDS. Two-thirds knew of sexually transmitted diseases and more than half (57 percent) of which mentioned AIDS as a sexually transmitted disease. A closer look at their knowledge of HIV/AIDS, however, shows that
misconceptions about the disease exist for a sizeable proportion of the youth population. While majority knew that AIDS can be contracted from a healthy-looking person and even from one single sexual contact, 35 percent agreed that the disease is a punishment from God for people who have sexual intercourse outside of marriage. Moreover, 28 percent said that AIDS is curable. Seventy three percent believed that only those with multiple sex partners are at risk of infection. Comparing the results from the 1994 YAFS survey, no substantial change in level of awareness of STD/HIV/AIDS was observed. However, the percentage of young adults who think that AIDS is curable more than doubled. In 1994, only 12.5 percent thought there is cure to AIDS. This study shows that there is a moderate level of knowledge on HIV/AIDS among Filipino youth. Across background characteristics, levels of awareness and knowledge show considerable variations in terms of age, gender, educational attainment and religion.
As the age increases, the level of awareness also increases. Older respondents are more knowledgeable about AIDS as shown by higher percentage among them who agreed that AIDS infection is possible even with a single sexual encounter and from a person who looks healthy. Young adults exhibit more risky sexual behaviors and has the greater number of HIV-AIDS cases than the adolescents. The population within the age range 15-24 continues to comprise the major bulk of HIV infections. Based on estimates by the UNAIDS, more than half of new infections belong to this age group (UN, 2002). According to Department of Health National Epidemiology Center (2011), young males are prone to engaging in health risk behavior without and more protection young females and are are also doing the same
prone to
aggressive or coercive to
behaviors of others in the community such that it often results
significant number of unwanted pregnancies, septic abortion and poor self-care practices. Laguna (2004) also stated that there is a noticeable gender difference on the knowledge of sexually transmitted diseases. More males than females are familiar with STD. Slightly higher percentage of females however said that AIDS can be contracted from a healthy
looking person (62 percent vs. 57 percent). But studies show that females have the greater level of awareness than males. Results also show that education reinforces knowledge
regarding HIV/AIDS. The percentage who believed that AIDS infection is possible through single intercourse and from a healthy looking person increases with level of educational attainment. Those with college education in particular appear to be knowledgeable on HIV/AIDS. The Churchs traditional opposition to sexuality and
reproductive health education in schools has affected what can be taught and how, thus affecting the quality of the information available to young people (Varga, C.A, 2003). In terms of religion, studies show that Catholics are generally more aware and knowledgeable about HIV/AIDS compared to those belonging to other religious affiliation. More Catholics are familiar with and have heard of AIDS and know that a healthy looking person can be a carrier of the virus. However, more youth from other religions (aside from Catholics, Islam and other Christian
denominations) know that a single sexual intercourse could lead to HIV infection (Laguna, E.P., 2004).
Independent Variables Variable
Dependent
Profile: Age Gender Educational Attainment Religion Level of Awareness on HIV-AIDS
Figure 1 Schema of the study showing the interplay between independent and dependent variables.
Statement of the Problem The study aimed to determine the level of awareness on HIVAIDS among out-of-school youth in Barangay Camaman-an, Cagayan de Oro City in the year 2012. This study specifically sought to answer the following: 1. What is the profile of selected respondents in terms of: 1.1 1.2 1.3 1.4 Age; Gender; Educational attainment; and Religion?
2. What is the level of awareness on HIV-AIDS of the respondents in terms of: 2.1 2.2 2.3 Transmission; Myths; and Preventive measures?
3. Is there a significant difference of the level of awareness on HIVAIDS when respondents are grouped according to: 3.1 3.2 3.3 3.4 Hypothesis Age; Gender; Educational attainment; and Religion?
Questions 1 and 2 are hypothesis-free. For Question 3 the following null hypothesis was formulated: Ho: There is no significant difference on the level of awareness when respondents are grouped according to: Age, Gender, Educational Attainment, and Religion. Significance of the Study The findings of this study are beneficial to the following: To the Current Researchers. The results give an idea of the recent level of awareness of the out-of-school youth. This will enable the researchers to convey this study to the proper authorities and motivate them to develop and promote programs. To Barangay Camaman-an. Being the chosen place for our study, the result of our research will served as an assessment of a timely social issue. This will provide an indicator to initiate appropriate government programs to increase level of awareness and prevention of HIV-AIDS. To Parents. Being directly concerned about the health of their children could benefit from the result of this study by being aware that there is a need for proper guidance to their child. As the primary provider, they may give supplementary teachings about sexual health and risks accompanying such practice.
10
To Out-of-School Youth, particularly the respondents of this study will be able to determine their level of awareness thus assisting them to do appropriate subsequent actions and assess the need for further information. To Barangay Health Workers. The results may give them an idea on the need for support and implementation of HIV-AIDS reduction programs and promote sex education to enhance their awareness in sexual health in their barangay. To Department of Education. By knowing the level of awareness of the out-of-school youth and to how far they understand about HIV-AIDS, they can take actions and plans on disseminating information about the disease and how to broaden the coverage of sex education to the out-of-school. To Department of Health. The result of the study may initiate them to conduct programs that will inform the public the fact about HIV-AIDS and eliminate misconceptions and myths. To Future researchers. Any researcher graduate or undergraduate can utilize this study in their quest for determining the level of awareness of the youth, specifically the out-of-school in a specific place. Findings of this study can also serve as a basis for future researchers to conduct related case.
11
Scope and Limitations of the Study The study focused on the level of awareness of out-of-school youth regarding HIV-AIDS. The respondents involved were those adolescents and young adults, aging 15-24 years old, who are not attending school. It was the objective of the researchers to
determine if they are well informed about important matters that concerns the welfare of the out-of-school youth in Barangay
Camaman-an, Cagayan De Oro City. The limitation of our study was on locating our respondents. Heiman (1999) defined out-of-school youth as hidden population. Aside from the number of out-of-school in is not known, finding them may not be easy. They may be highly diffused all over the Barangay. Therefore, the researchers gave ample amount of time to look for respondents and gathered all the data. Definition of Terms Age. The entire period of life or existence of a person (Websters Comprehensive Dictionary, 1996). In this study, it is divided in two groups: adolescents (15-19 years old) and young adults (20-24 years old). AIDS (Acquired Immunodeficiency Syndrome). Caused by HIV; sets a point in the continuum of HIV pathogenesis in which the host
12
has clinically demonstrated profound immune dysfunction (Smeltzer and et al, 2010). It is a pandemic disease wherein everyone especially the youth is vulnerable of acquiring it. Educational Attainment. It is an accomplished instruction or training in an institution of learning (Websters Comprehensive Dictionary, 1996). It refers to the highest educational level attained by the respondent. This may be categorized as elementary level,
elementary graduate, high school level, high school graduate and college level. Gender. Corresponds to sex, animate beings are either masculine or feminine. (Websters Comprehensive Dictionary, 1996) It refers to the respondents of this study, either/whether male or female regarding HIV-AIDS awareness. HIV (Human Immunodeficiency Virus). The causative agent of AIDS. It is transmitted through sexual contact or percutaneous injection of contaminated blood or from infected mother to fetus (Smeltzer and et al, 2010). It is the virus, causing Acquired Immunodeficiency Syndrome that came from any group of retroviruses and inhibits the immune
13
system, leaving a person vulnerable to a variety of fatal diseases. Level of Awareness. It is the degree of knowledge or consciousness (Websters Comprehensive Dictionary, 1996). It refers to the extent of the awareness of the out of school youth regarding HIV-AIDS measured using a survey method. It is categorized as highly, moderately, fairly aware or unaware. Out-of-School Youth. The young who are in the state of being away or not attending school (Websters Comprehensive Dictionary, 1996). It refers to the adolescents and young adults, aging 15-24 years old, who are not attending school, who will be the respondents of this study. Religion. It is a system of faith and worship (Websters Comprehensive Dictionary, 1996). It refers to the denomination and beliefs of the respondents whether Catholic, Islam, Protestant, Seventh Day Adventist, or others. CHAPTER 2 REVIEW OF RELATED LITERATURE AND STUDIES
Although progress has been made to treat the incurable
14
Human
Immunodeficiency
Virus
Acquired
Immunodeficiency
Syndrome (HIV-AIDS), the epidemic remains a critical public health issue in all communities across country and the world (Brunner & Suddharth, 2008). In this study, the chosen respondents are those have higher risk of acquiring this disease. Many evidences showed that the youth, especially the out-of-school are vulnerable in acquiring HIV-AIDS. HIV-AIDS is a new disease: it was first described in 1981 (LeVay, 2006). The epidemic began spreading in 1980 in North America, and has quickly reached all corners of the globe. The Centers for Disease Control and Prevention (2003) reported that there are more than 20 million died from HIV-AIDS globally. In the epidemic report of Joint United Nations Programme on HIV/AIDS (UNAIDS) and World Health Organization (2003), this disease killed up to 3.5 million people in 2003 alone and infected up to 5.8 million others. Also, WHO Western Pacific Regional Headquarters (2003) account that in Asia, an estimated 7.2 million adults and children are living with HIV. In 2002, UNAIDS reported that each day about 16,000 people become newly infected with HIV, or 11 men, women and children per minute. 11 percent of the newly infected people are under 15, over
15
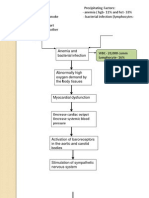
50 percent of new infections are now occurring in people between ages 15 and 24, primarily due to sexual infection. According to Bagsao, The 2010 Global AIDS report on the killer diseases situation remains unchanged. That is, the Philippines is still one of only seven countries in the world have recorded a sharp increase in the number of HIV cases. From an estimated 600 HIV case`s in 2001, some 4,600 new infections were monitored by the Department of Health last year (Philippine Daily Inquirer, April 04, 2012). Progression of HIV Infection The human immunodeficiency virus (HIV), which causes AIDS, is transmitted through bodily fluids (mainly blood and semen), usually by sharing intravenous drug needles or by sexual contact with an infected partner. The virus attacks the bodys immune system, leaving a person vulnerable to a variety of fatal diseases (Papalia, 2006). HIV follows a complex course after it enters the body. Most people who are infected with HIV exhibit no early symptoms. When they do occur, they appear within a month or two from exposure and manifest flu-like symptoms such as fever, headache, fatigue, and enlarge lymph nodes. When symptoms do occur, they generally
16
resolve within a week or month. Nevertheless, infected individuals are highly contagious during this time. Initial infections are generally followed by an asymptomatic period that may last anywhere from several months up to ten years. During this time the virus multiplies and begins destroying the cells of the immune system is compromised and cannot mount defenses for opportunistic infections and diseases. AIDS is the term used to describe advanced stages of HIV infection. Symptoms include coughing and shortness and breath, seizures, difficulty in
swallowing, mental impairment, diarrhea, fever, nausea, abdominal cramps, weight loss, severe fatigue, loss of vision and death. HIV-AIDS in the Philippines In 1988, an anecdotal report indicates that one infected Filipina prostitute from New York City came home to die in the Philippines. Twenty years after AIDS was diagnosed in California, the first twenty cases of AIDS were diagnosed in the Philippines (1990). Epidemiologists believe a major factor in the spread of HIV is the U.S. military personnel who frequented the sex bars and bordellos in the towns surrounding Clark Air Force Base and the Naval Base in Subic Bay. In 1992, it was estimated that 234 people were infected; by 1994, there were 834 cases.
17
According to L. B. Duchene (1997) of Doctors without Borders (Mdicins Sans Frontires), 1,234 Filipinos were infected with the AIDS virus in 1997. But the World Health Organization (WHO) estimated that the true figure of Filipinos with AIDS in 1998 was approximately 23,350 persons. The dramatic increase in AIDS cases is attributed by MSF to exposure and infection of the virus through prostitution (heterosexual activities), the prohibitive cost of
medicines, malnutrition, economic depression, untreated STDs, and limited access to modem medical care. Contrary to the experience in the industrialized nations, mortality is almost 82 percent in the first year of infectivity and 98 percent in two years. WHO and MSF estimate the Philippines will have 30,112 cases by the end of 1999, and about 39,780 cases by the year 2000. That is a 70-percent increase in the incidence of AIDS in just two years in a population of 79 million people. The DOH National Epidemiology Center (2011) reported that from 1984 to 2011, there were 860 AIDS cases reported, 71 percent (613) were males. Of the reported AIDS cases, 323 (38 percent) had already died at the time of case reporting. Sexual contact was the most common mode of HIV transmission, accounting for 93 percent (799) of all reported AIDS cases. The number of HIV cases continues
18
its upward trend, with the latest figure in January 2011, there were 152 new HIV Ab sero-positive individuals confirmed by the STD/AIDS Cooperative Central Laboratory (SACCL) and reported to the HIV and AIDS Registry. This was a 6 percent increase compared to the same period last year. Most of the cases (93 percent) were males. In an ABS-CBN News TV Patrol episode last June 19, 2012, HIV in the Philippines is now epidemic. There is an average of ten (10) Filipinos develop new cases of HIV per day. As of January 2012 there were 313 new cases of Human Immunodeficiency Infection. The new cases affected are those within the age range of 20 and 29 accounting to 61 percent (129). The DOH has recorded a total of 8,576 HIV cases since 1984. Of these cases, 975 patients are already suffering from acquired immune deficiency syndrome (AIDS), while 345 had already died. According to STD/AIDS Cooperative Central Laboratory
(SACCL), this year's figure is a 72-percent increase. In the February 2012 update, all cases acquired the infection through sexual contact - one homosexual and five bisexual. ''Of the 486 HIV positive cases in 2012, twelve were reported as AIDS cases. All were males. Ages ranged from 7 to 47 years (median 35 years) and 92 percent acquired the infection through sexual contact - five homosexual and
19
six bisexual contacts. The other mode of transmission include one mother-to-child transmission,'' the registry said (Manila Bulletin, March 25, 2012). According to Dr. Jerie P. Calingasan, Cagayan de Oro City Health Officer, there are 31 reported cases of HIV-AIDS throughout the city. He exclaimed that there is really a need for the promotion of HIV-AIDS awareness not only to specific groups but to everyone because all are susceptible in acquiring HIV. Youth at Risk This growing threat of HIV/AIDS infection concerns particularly the youth. According to UNFPA (2011), young people are at the centre of the global AIDS epidemic. Of the 1.7 billion young people worldwide, 5.4 million are estimated to be living with HIV (2007). About 40 percent of new HIV infections are among young people. This age group also has the highest rates (over 500,000 infections daily) of sexually transmitted infections excluding HIV. They are considered to be at particular risk for HIV infection because many of them engage in high-risk behaviors, believing they are invulnerable to infection (Allender, J.A., Rector, C., and Warner, K.D., 2010). Worldwide, they are considered one of the more vulnerable segments of the population insofar as HIV/AIDS infection is
20
concerned. The population within the age range 15-24 continues to comprise the major bulk of HIV infections. Based on estimates by the UNAIDS, more than half of new infections belong to this age group (UN, 2002). The vulnerability of young people to sexually
transmitted infection is associated with their growing involvement in risk behaviors such as early and unprotected sex, having multiple partners, drug use and alcohol abuse. Recent statistics on adolescent sexuality in the Philippines point to an increasing number of youth engaged in premarital sexual intercourse and other risky sexual practices (Raymundo, Xenos, & Domingo, 1999; Natividad & Marquez, 2004). Based on the recent adolescent survey, premarital sex (PMS) prevalence among youth aged 15-24 rose from 18 percent in 1994 to 23 percent in 2002. Majority of these sexual experiences are spontaneous in nature, and in most instances, unprotected. There is also liberalizing views on sex among the young. In 2002, 34 percent of Filipino youth approved of men having PMS while 22 percent approved of the same behavior for women. Approval of PMS for women almost doubled in 2002 from the 13 percent approval posted in 1994 (Ventura & Cabigon, 2004). However, as more people are engaging in sex at earlier ages, they do so lack of sufficient information on reproductive health,
21
particularly, the consequences of early sex (Zablan, Marquez, & Laguna, 2003). The sexual behavior of the youth is a source of current concern. In fact, probably there is no other area of adolescent sociopsychological problems about which society has as much uneasiness (Josselyn, 1971). For Seigel (2006), during adolescence, the self or basic personality, is still undergoing a metamorphosis and is vulnerable to a host of external determinants. It is a time of trial and uncertainty for many youths. LeVay (2006) considered adolescence as time of sexual exploration. This period is marked by a great increase of sexual feelings and often accompanied by an increase in sexual behavior. HIV/AIDS, pose serious threats for all sexually active people, but they constitute a particular risk to the youth due to physical, psychological and social factors. Often, the youth do not understand how to protect themselves against sexually transmitted diseases. Because most societies frown on premarital sex, young people may be embarrassed to seek help and may be turned away if they do. Evidence suggests that adolescent women constitute the sex and age group most susceptible to HIV infection. Young women are physiologically more vulnerable to STDs and also more vulnerable to
22
coercion. Social reasons for increased risk of HIV and exist on different levels. Some relate directly to the situations in which adolescents are put at risk such as unequal relationships because of the low status of women, young people and the poor. Examples of this are manifold and include sexual abuse, incest and situations where the woman is not able to determine when and how to have sexual intercourse. Sexually transmitted diseases are also transmitted because of to the failure or inability to negotiate contraceptive use, promiscuous behaviour by partners, relationships involving money for sexual favours ("Sugar Daddies" or "Sugar Mommies") and fulltime prostitution. From 75 to 85 out of every 100 HIV infections are transmitted through unprotected sexual intercourse, but the virus also spreads through mother-child transmission, blood transfusion and drug use. The latter constitutes a particular danger for young people. Tobacco, alcohol and other drugs are readily available to most young people. In the modern world, these substances constitute a real danger to adolescent health in both the short and long term. Their use has been linked to high rates of STD and HIV transmission (UNFPA, 2011).
23
Increased Vulnerability of Out-of-school Youth Knowing that the youth are susceptible in getting HIV-AIDS, being out-of-school increases the risk. Burns, A.A. (2004) stated that across the globe, out of school youth are a diverse group. They may have completed school, dropped out, or never started school. Mainstream out of school youth includes married adolescents, boys and girls in rural areas and girls who get pregnant and have to leave school. In Young Adult Fertility and Sexuality Survey, PEARHPP Report (1994), the highest percentage of those reported STD symptoms come from the out-of-school youth among other groups, which are the in-school and working youth. Also, DOH mentioned that the Filipino youth are vulnerable to STDs especially the out-ofschool, street-dwellers, and urban-based youth for they posses high risk sexual behavior. Stine (2002) affirmed that youth dropouts have higher frequencies of behaviors that put them at risk for HIV/STDs and are less accessible to prevention efforts. Compounding the challenge, in the name of morality, culture or religion, young people are often denied their right to education about the health risks of sexual behaviors and to important tools and services for protection. Among the worlds young people, some are more exposed to HIV than
24
others. Those are living in what UNICEF terms, especially difficult circumstances include young people who are out of school, who live on streets, who share needles with other infecting drug users engage in commercial sex or who are sexually and physically abused. Muss (1998) suggests that these out-of-school youth are more likely to be sexually active and to have sexual intercourse at an earlier stage, to have had a greater number of sexual partners, to have elevated rate if unintended pregnancies, sexually transmitted diseases (STDs) and alcohol or other drug abuse. Contraceptive use, including use of condoms during sexual intercourse, is the exception rather than the norm in this population. According to Rep. Arnel Ty of the LPG Marketers Association (LPG-MA), a growing number of Filipinos have been infected with the human immunodeficiency virus (HIV) as a result of using injecting drugs with contaminated needles. Of the 1,032 new HIV infections from January to April, at least 96 cases, or 9.3 percent, were due to injectable drug use (IDU) (Philippine Daily Inquirer, June 10, 2012). According to the National Statistics Office Annual poverty indicators survey of 2010, there are 6,065,000 (16 percent) Filipinos aging 6-24 years old are out-of-school-youth. For out-of-school youth
25
aged 18 to 24, looking for work was also cited as a main reason among males, and marriage, among females. In Northern Mindanao (Region X), out of estimated 1,835,000 Filipinos aging 6-24 years old, 17.3 percent are out-of-school-youth. According to Sunstar Cagayan de Oro published last November 9, 2011, Northern Mindanao ranks forth with high number of out-of-school youth. In the Encyclopedia of Sex and Gender (2006), the larger role of the schools in sex education is important in educating the youth and preparing them for the responsibilities that come with sexual maturation. Sexual education programs can help the youth make better-informed choices about sexuality. Sexual education in the schools is compelling in the light of the sexual practices of youth and resulting social, health, and economic consequences. Studies have shown that sexual behavior starts later among youth who are religiously observant and who are of higher intelligence. More intelligent youths may be more occupied with educational and other career-related activities and thus have less time for sexual
relationships (LeVay, 2006). This just means that in-school youth have reduced risk in contacting HIV-AIDS than that of out-of-school. Prevention Strategies Without a vaccine available to protect against HIV, the major
26
focus of preventive efforts at the individual, dyadic and social network levels are designed to minimize the transmission of HIV through unsafe sexual practices and the sharing of contaminated injection drug equipment. A number of methods have been developed and scientifically shown effective in reducing risky behavior when applied under specific conditions. These methods include indigenous leader and peer outreach strategies, prevention case management, needle hygiene and syringe distribution
programs, social support group organized around risk reduction, and Internet intervention. At the health services level, prevention efforts focus primarily on promoting HIV counseling and testing, offering therapy for HIV-positive pregnant women and their infants,
continued stringent screening of all products used medically by blood transfusions and appropriate protection of health care workers. A total of 313 Filipinos were diagnosed with HIV last March, contributing to a rise of a total of 799 cases for the first three months of the yeara 65 percent rise from last year's 483 cases in the same quarter. This alarming number is one of the reasons why the Aquino administration should certify as urgent the passage of House Bill 5312, a proposed new AIDS Prevention and Control Law.
27
The new legislation has become absolutely imperative to effectively suppress the HIV epidemic, said LPG Marketers Association Rep. Arnel Ty. The bill seeks to earmark P400 million to jumpstart a new National HIV and AIDS Plan (Manila Bulletin, May 02, 2012). The process of "partner notification" is gaining increasing attention for preventing the spread of infection from patients with diagnosed HIV to healthy persons. Through this process, sex and needle partners of index patients are informed of their possible exposure to infection and the need for medical evaluation. Treatment As of now, AIDS is incurable, but increasingly the related infections that kill people are being stopped with antiviral therapy, including protease inhibitors. Many HIV-infected people lead active lives for years. Because symptoms may not appear until a disease has progressed to the point of causing serious long-term
complications, early detection is important. Regular, school-based screening and treatment, together with programs that promote abstention from or postponement of sexual activity, responsible decision-making and ready availability of condoms for those who are sexually active may have some effect in controlling the spread of STDs. Most young people who find out that they have HIV change
28
their sexual behavior, and half stop injecting drugs (Papalia, 2006). Treatment modalities for HIV are rapidly changing as a result of scientific research. No single medical regimen is universally
accepted, although some are now preferred for initial therapy. At the time of this writing the Food and Drug Administration has approved the use of 20 different drugs to combat HIV infection- often in some form of combination. These drugs fall into four main types: Nucleoside and nucleotide analog reverse transcriptase inhibitor which inhibits HIV's ability to copy a healthy cell's DNA. HIV needs the cell's DNA, or genetic instruction, to replicate itself and without complete DNA, HIV cannot make new copies. Nonnucleoside reverse transcriptase inhibitor also prevents HIV from using a healthy cell's DNA to make copies of itself, but they have different mechanism of action. Protease inhibitor prevents infected cells from releasing HIV into the body. Fusion inhibitor prevents entry of HIV virus into healthy cells (Bickenbach, 2006).
Level of Awareness on HIV-AIDS Indeed, determining the level of awareness of these out-ofschool youth about HIV-AIDS is very relevant. There are studies
29
shown that the youth has low awareness and have misconceptions about this deadly and prevalent disease. The YAFS survey of DOH showed that the proportion of those who think AIDS is curable more than doubled (from 12 percent in 1994 to 28 percent in 2002). Many adolescents also resort to services of unqualified traditional healers, obtain antibiotics from pharmacies or drug hawkers or resort to advices from friends (e.g. drinking detergent dissolved in water) without proper diagnosis to address problems of STDs. Improper or incomplete treatment may mask the symptoms without curing the disease increasing the risk of transmission and development of complications. The limited use of condoms to protect adolescents from risk of HIV is an issue to reflection for condom use is not only to prevent pregnancy but also STDs. Awareness of HIV-AIDS is near universal at 95 percent, yet only 27 percent think there is a chance of them getting AIDS. Predictably, HIV/AIDS and STI awareness is higher in urban areas, among bettereducated classes, and among older youth (20-24) versus the younger (15-19). According to Rathus (2008), studies regarding knowledge, attitudes, and beliefs about HIV/AIDS find that even children in the early school years are aware of HIV/AIDS. Nearly all high school
30
students know that HIV/AIDS is transmitted by sexual intercourse, but about half do not modify their sexual practices as a result of fear of the disease. Adolescents often deny the threat of HIV/AIDS to them. The hotline counselor says that some teens are unfazed when they test positive. Adolescent males may even consider STIs to be warrior marks, proof of their sexual prowess. The first concern of younger callers those 16 and below who consult the hotline because they suspect they have been infected is not their own health but how they could win back their girlfriends or boyfriends. They dont see its a serious problem, notes the counselor (PCIJ, 2010). In a study presented to 2004 Annual Meeting of the Population Association of America, the results show that: Regarding the age, 2024 years old has an increased level of awareness than those 15-19 years old. In terms of gender, females have the greater level of awareness. Education reinforces knowledge regarding HIV/AIDS. The percentage who believed that AIDS infection is possible through single intercourse and from a healthy looking person increases with level of educational attainment. Those with college education in particular appear to be knowledgeable on HIV/AIDS. In terms of
31
religion, Catholics are generally more aware and knowledgeable about HIV/AIDS compared to those belonging to other religious affiliation. More Catholics are familiar with STD, have heard of AIDS and know that a healthy looking person can be a carrier of the virus. However, more youth from other religions (aside from Catholics, Islam and other Christian denominations) know that a single sexual intercourse could lead to HIV infection. By and large, there is a moderate level of knowledge on HIV/AIDS among Filipino youth (Laguna, 2004). Incomplete information about HIV/AIDS can both elevate HIV risk and fuel negative stereotypes about people living with the disease. In July 2002, a joint report of UNAIDS, WHO and the United Nations Childrens Fund (UNICEF) stated that the vast majority of people aged fifteen to twenty-fouran age group that accounts for 50 percent of new HIV infections worldwidehad no idea how HIV/AIDS is transmitted or how to protect themselves from the disease. Only about 25 percent of sexually active inner-city adolescents use condoms correctly and regularly, despite knowing how AIDS is transmitted. These data reveal a high rate of unsafe heterosexual behaviors among adolescents, and particularly among inner-city
32
minority youths. They suggest that abstinence and safe sexual practices must be fostered through programs aimed at this population. Thus despite adolescents having accurate knowledge about HIV/AIDS risk, both male and female adolescent revealed that they either continued to take risks in their sexual behavior or that they began to practice more risky behaviors as they got older (Franklin, N. et al, 1995). In adolescents, HIV/AIDS related knowledge has been found to be variable. Keller et al( 1991) found that knowledge concerning HIV transmission, methods of prevention of HIV transmission, and general knowledge concerned with AIDS was high for all inner-city minority adolescents in one sample (both sexually active and inactive). The importance of HIV/AIDS related knowledge, however, is its potential impact on behavior. The youth are at a risk, not only because of biologic reasons but also because of the immaturity of their knowledge and practice of sexual health. They are often sexually active. While school and other education programs try to prevent initial infection, additional opportunities to prevent re-infection are not fully utilized (Faro and Soper, 2001). Educating the Youth
33
Young people are particularly vulnerable to HIV infection for social, political, cultural, biological, and economic reasons. Whatever their circumstances, in order to protect themselves against HIV, young people need information, skills, truth-friendly health services and a safe and supportive environment (UNFPA, 2011). For Rathus (2008), prevention and education are the primary weapons against HIV/AIDS. Adolescents need to learn about the transmission, symptoms, and consequences. They need to learn about safer sex techniques, including abstinence, and, if they are sexually active, the use of condoms. Educating young people to use condoms is associated with lower levels of infection. But knowledge alone may not change behavior. For example, many female adolescents lack power in their relationships. Males are likely to pressure them into unwanted or unprotected sexual relations. Other goals of educational programs should include enhancing the adolescents sense of control over the prevention of AIDS and modifying behavior associated with being infected with HIV. The goal of educating people about STDs such as HIV-AIDS is to convince them to change their behaviour when it comes to risky sexual practices. According to Stine (2002), the problem with AIDS education is that communicating the information is relatively easy
34
but changing behavior, particularly addictive and pleasurable behavior, is quite difficult. This is difficult in all population, but presents special challenges when working with adolescents. Besides being biologically more susceptible to HIV-AIDS, many social and developmental influences create barriers to safe behavior in this age-group. Some teens cannot complete a task requiring multiple steps (physically using a condom correctly). Egocentrism often leads teens to believe they can tell who has an STD and who is safe. A successful HIV-risk reduction program developed with teen input included colorful posters, pocket calendars for participants (Black, J. & Hawks, H., 2005). For Stine (2002), the goals of educating people about HIV infections and AIDS are to promote compassion and social
understanding and to prevent HIV transmission. To achieve this goals, accurate information must be provided that makes people aware of their risk status. People at minimum risk can continue their safer sexual lifestyles. People at high risk should determine their HIV status, alter behaviors and practice safer sex. A number of social, cultural and attitudinal barriers continue prevent the implementation of promising HIV risk-reduction programs. The remote prospects for a successful prophylactic vaccine for HIV and the difficulty in finding
35
long-lasting
effective
drug
treatments
have
underscored
the
importance of sustained attention to HIV prevention and education. Generally, Filipinos are sexually conservative. According to Lu (2004), this conservatism hampers the sex education and
information initiatives because sex is considered taboo and is not discussed openly, especially not with the youth. It also prevents people from seeking sexual advice or health care because of the embarrassment of having to do so, this leads to self-medication at best, or worst, not seeking care at all. There are government and non-government agencies that promote programs for the youth. Example is the Population Awareness and Sex Education for Out-of-school Youth Program, making the youth, especially the out-of-school to be prepared in becoming responsible citizens, aware of the consequences of rapid population growth and the importance of sex education (Population Education, 1977). The WHO supports the development of national AIDS
prevention and control programs in more than 120 countries throughout the world. In addition, it collects information about cases and maintains a virus bank (because AIDS viruses from different parts of the world can vary somewhat in their biochemistry). Finally,
36
it makes recommendations on international travel and related issues and serves as a forum for discussing the scientific and practical implications of the AIDS pandemic. There is also a domestic law in the Philippines which is the Republic Act No. 8504 - Philippine AIDS Prevention and Control Act. Stated in section 2, the gravity of the AIDS threat demands strong State action today, thus: the State shall promote public awareness about the causes, modes of transmission, consequences, means of prevention and control of HIV/AIDS through a comprehensive nationwide educational and information campaign organized and conducted by the State. Such campaigns shall promote value formation and employ scientifically proven approaches, focus on the family as a basic social unit, and are carried out in all schools and training centers, workplaces, and communities. This program shall involve affected individuals and groups, including people living with HIV/AIDS. The State shall extend to every person suspected or known to be infected with HIV/AIDS full protection of his/her human rights and civil liberties. Towards this end: compulsory HIV testing shall be considered unlawful unless otherwise provided in this Act; the right to privacy of individuals with HIV shall be guaranteed;
37
discrimination, in all its forms and subtleties, against individuals with HIV or persons perceived or suspected of having HIV shall be considered inimical to individual and national interest; and provision of basic health and social services for individuals with HIV shall be assured. The State shall promote utmost safety and universal
precautions in practices and procedures that carry the risk of HIV transmission. It will positively address and seek to eradicate conditions that aggravate the spread of HIV infection, including but not limited to, poverty, gender inequality, prostitution,
marginalization, drug abuse and ignorance.
The State shall
recognize the potential role of affected individuals in propagating vital information and educational messages about HIV/AIDS and shall utilize their experience to warn the public about the disease. Article 1 states that access to complete HIV/AIDS information in the countrys schools, health facilities, work places, pre-departure seminars for overseas workers, tourist destinations, and local communities is guaranteed. It is now clear that any plan to decrease the social and economic impact of AIDS in the Philippines, as in any society, requires an emotional engagement that facilitates an important
38
paradigmatic change of beliefs and behavior. This paradigmatic change is essential to practicing abstinence, to increasing the use of condoms, decreasing promiscuity, promoting the use of disposable needles among drug addicts, understanding and respecting those who suffer, and helping individuals everywhere to enjoy sexuality while minimizing the risks for ones self and society. In addition to emotional engagement, changes in individual attitudes require the active and creative support of social groups to which the individual belongs; namely families, schools, private businesses, and churches. In 1995, a private-civic organization hired Magic Johnson, a famous American basketball superstar, to give talks to Filipino youth about HIV prevention and living a responsible and healthy sex (safe) life. To ensure the well-being of the youth, all must aggressively pursue the education, follow-up education, and, even more
importantly, the follow-up counseling of adolescents, who are at the stage in life during which they are least receptive to adult interventionwhen they are confronted with adulthood themselves, an adulthood that includes the challenge and excitement of sex and drugs. To ensure and encourage stable environments and
compassionate care, family members and communities must be
39
educated to respond to those in need of care. Family case management is critical, but existing informal networks must also be encouraged. Only such steps will help kill the climate of fear about AIDS (Crimp, 1989).
Summary HIV-AIDS is a progressive and widespread disease that
40
everyone should be aware of. It can be acquired by anybody especially those who have high-risk behaviors. In the case of this study, the vulnerable youth, particularly the out-of-school, should be responsible enough and conscious of all their actions regarding the promotion of their health and lifestyle.
CHAPTER 3 RESEARCH METHODOLOGY
41
Research Design This study used the descriptive survey design which has been designed to give a picture of out-of-school youth's level of awareness towards HIV-AIDS. The descriptive survey method was employed for the purpose of suitably describing these ideas, beliefs, and attitudes as well as to pinpoint the connection between the factors and the characteristics of the object. It also aimed to determine, describe and analyze the difference in the dependent variable when grouped according to independent variables. Research Setting This research study was conducted at Barangay Camaman-an. It is composed of fifteen (15) sitios, namely: Bolonsori, Bontong, Macajalar, Pinikitan, Tipolohon, Macapaya, Sta. Cruz, Ramonal Village, Patrick Cronin Village, Central Village, Pallawan, Tierra del Puerto, Upper Bontong, Centro Camaman-an and Adela. Barangay Camaman-an has a land area of 743.86 hectares and an estimated population of 23,350. It is about two kilometers the urban center of Cagayan de Oro. The barangay has a forty-eight classroom elementary school, a National High School, both government-owned and those that are privately managed. According to the Department of Education, Camaman-an
42
National High School ranked 15th among all the 35 public secondary schools in Cagayan de Oro City in terms of highest drop rate which is 5.53 percent in the school year 2009-2010. In 2011, the drop rate increased to 7.77 percent which shove them to the 9th rank. Aside from being a part of Xavier University community, Barangay Camaman-an was chosen in terms of its total population, which has a larger number compared to the others which ranked higher than Camaman-an. It is considered as one of the barangays that has the highest number of out of school youth in Cagayan de Oro City. There are estimated 1,142 out-of-school youth in Barangay Camaman-an. In fact, Xavier University signed a Memorandum of Agreement with SMART Communications Inc, Philippine Business for Social Progress (PBSP), and the Department of Education (DedEd) Region 10 for CommuniTeach, a project seeking to reduce dropout rates in public elementary schools. One of the beneficiaries of this project was Camaman-an Elementary School.
Respondents and Sampling Procedure Heiman (1999) defined out-of-school youth as hidden
population. The exact number of out-of-school youth in Barangay
43
Camaman-an is not known. According to the November 9, 2011 issue of SunStar Cagayan de Oro, the percentage of out-of-school youth aging 6-24 years old in Northern Mindanao is 17.3 percent and the youth population (15-24) of Barangay Camaman-an is 6,599. The estimated total population of out-of-school youth is about 1,142. The calculated sample size is 288. The sampling method used for this study was the nonprobability sampling method snowball or network sampling. It is an approach wherein, early sample members are asked to identify and refer other people who meet the eligibly criteria for study. After observing the initial subject, they were able to identify people with a similar trait of interest. The researchers then observed the nominated subjects and continued in the same way until the obtaining sufficient number of subjects. This type of sampling technique works like chain referral. This is used when the population consists of people with specific traits who might be difficult to identify by ordinary means. The inclusion criteria for this study were all out-of-school youth in Barangay Camaman-an, ages ranging from 15-24 years old both female and male. The exclusion criteria were subjects that are outside of those criterions (Polit and Hungler, 1993).
44
Research Instruments The researchers of this study utilized a modified questionnaire from United Nations - Economic and Social Commission for Asia and the Pacific, Social Development Division of 2009. This was validated by Miss Rosario Lei M. Pasimio, RN, a staff nurse from Polymedic Hospital, Dr. Victoria O. Galang, MD, an Ob-gyne physician and Dr. Mercy Dita L. Eduave, MD, a pediatrician; both physicians are from Bukidnon Provincial Medical Center. Questions were framed in a way that was easy to understand using Visayan language. Difficult technical terms were avoided in the preparation of the questionnaire. The Visayan translation was validated by Mrs. Susie Serrano, a Filipino and Values Education secondary teacher in Lapasan National High School. The first part of the questionnaire is the respondents profile and the second part measures their level of awareness on HIV-AIDS by answering a 20-item test. This research instrument was subjected to pilot test to twenty (20) out-of-school youth in Divisoria, Cagayan de Oro City and was proven valid and reliable with value Cronbach alpha. Scoring Procedure The questionnaire is composed of 2 parts. Part 1 dealt with 0.725
45
information on the demographic profile of the respondents such as name, age, gender, educational attainment and religious affiliation. In determining the level of awareness in part 2, 20 questions are answerable by Agree, Disagree and Not Sure. Likert scale method was used in the study. The Likert Scaling Technique assigns one scale value of each of the different responses. Every response has an equivalent point from 1 to 3; then points are summed up. To interpret the responses to a Likert Scale, each category is assigned to a numerical value such as Highly aware as 3, Moderately aware as 2 and Unaware which is equal to 1. The total assigned value was determined by using the arithmetic mean. The score was then interpreted as Highly Aware, Moderately Aware, and Unaware. ARITHMETIC MEAN 2.34-3.00 1.67-2.33 1.00-1.66 Data Gathering Procedures The researchers, along with a letter, met the Barangay Captain and asked for permission to conduct a survey in their barangay. After giving his consent to gather all the needed samples, the researchers scattered to the sitios and started locating the out-of-school youth SCALE 3 2 1 INTERPRETATION Highly Aware Moderately Aware Unaware
46
last June 2, 2012 at the internet cafs, stores, basketball courts, and other establishments that they might stay. Then, the researchers proceeded to drawing out the samples for the research, following the non-probability sampling method snowball or network sampling techniques. A consent form was given and signed by the qualified respondent. A survey questionnaire was then administered. The respondents were given at most ten minutes to answer the questionnaire for understanding and appreciation. The respondents were allowed to ask questions the initial for any clarification on the the
questionnaire.
After
respondents
answered
questionnaire, the researchers asked for assistance to help identify people with similar qualifications. The researchers tallied and tabulated the collected data for analysis and interpretation.
Statistical Tools The data collected in this study was subjected to certain statistical treatments. The data were coded, tallied and tabulated for better presentation and interpretation of the results. The statistical tools used were the following: Frequency and Percentage
47
The percentage and frequency distributions were used to classify the respondents according to their age, gender, educational attainment and religion. The frequency presented the actual
response of the respondents to a specific question or item in the questionnaires. The percentage of each item was computed by dividing it with the sample total number of respondents who answered the survey. Arithmetic Mean It is defined as the sum of the given data divided by the number of data. This was used to determine the average level of awareness in terms of HIV-AIDS transmission, myths and preventive measures. Also, it is utilized in the differences on the level of awareness when grouped according to profile.
Standard Deviation It is defined as the positive square root of the arithmetic mean of the squares of the deviations of the given values from arithmetic mean. It is used in the specific questions 2 and 3 to determine the homogeneity of the responses. T-test
48
A t-test was used when comparing two variables with normal distribution in table 9 which is the differences in level of awareness of HIV according to age. F-test An F-test was used to determine the significance of the differences between categories beyond two levels with normal distribution. Thus, it is used in table 12 which is the differences in level of awareness of HIV according to religion. Kruskal-Wallis test It is a non-parametric method for testing two or more samples. It is used in the study because the distribution is not normal or skewed. Thus, it is used in table 11 which is the differences in level of awareness of HIV according to educational attainment.
Mann-Whitney test It is a non-parametric statistical test that compares two samples under the independent variable. Utilized in the differences in level of awareness when grouped according to gender (table 10), this test was used instead of t-test since the graphical presentation showed a skewed distribution.
49
CHAPTER 4 PRESENTATION, ANALYSES AND INTERPRETATION OF DATA This chapter deals with the presentation, analyses, and interpretation of data gathered and collected through the use of the research instrument, which is a questionnaire. Following the order of the statement of the problem in chapter 1, the results were presented in tables with discussion.
50
Problem 1: What is the profile of selected out-of-school youth in
terms of:
1.1 1.2 1.3 1.4
Age; Gender ; Educational attainment; and Religion?
Table 1 presents that majority of the respondents (54.9 percent) were from adolescent group aging 15-19 years old, which means that incidence of drop out from school are prevalent from this age group. It is at this age when many of them become delinquent and exhibit attention-getting behaviors, leading them to be pulled out from school. It is also at this age when they finish their secondary education, thus making them more qualified to enter a job instead of continuing higher education. The Commission on Higher Education (2008) statistics
revealed that among the 66 enrolled in first-year, only 43 finish high school and from this number, only 23 enroll in college. In addition, Schmeer (2009) also supports that in the Philippines, schooling delays and early drop out are prevalent, as household duties and work responsibilities often force children out of school prior to high school graduation.
51
Table 1: Distribution of Respondents According to Age Age 15-19 20-24 Total Frequency 158 130 288 Percent 54.9 45.1 100.0
In the distribution of respondents according to gender, as presented in Table 2, more than half of the respondents were male, comprising to 59.7 percent. This implies that males are more likely to become an out-of-school youth than females. They are more exposed to peer pressure and engage in high-risk behaviors such as alcoholism, drug abuse, sexual promiscuity and rebellion. Males may also opt to drop out because of more availability of manual labor jobs than females. This finding is congruent to the trend of the Annual Poverty Indicatory Survey National Statistics Office of 2008, which states that out of an estimated 2.9 million children aged 5 to 15 years old who are out-of-school, about 1.7 million are boys and around 1.2 million are girls. In addition, Albert (2012) estimated that a higher rate of boys (13.3 percent) of secondary school age is out of school compared to girls (7.6 percent). According to Kaufmann (2006), males have a higher tendency to be pulled out from school due to
52
reasons of short term opportunities and tendencies of threatening behavior. Table 2: Distribution of Respondents According to Gender Gender Male Female Total Frequency 172 116 288 Percent 59.7 40.3 100.0
In the distribution of respondents according to educational attainment, Table 3 showed that majority of the respondents were high school graduates at 47.9 percent. Most of the respondents were able to attain until high school, since basic education is freely provided by the government. Economically-wise, their families can send them to school but no longer up to college where the cost is quite expensive; thus they tend to drop out from school after high school graduation and find work opportunities instead. According to an article in the Philippine Inquirer (2009), there is an increasing cost of education due to incessant tuition increases every year, thus, the dropout rate has worsened over the years as school-aged children are compelled to work and help their parents earn money for their familys daily expenses. These data clearly supports the educational attainment distribution of the out-of-school-youth.
53
Table 3: Distribution of Respondents According to Educational Attainment Educational Attainment Elementary level Elementary graduate High school level High school graduate College level Total Frequency 14 21 80 138 35 288 Percent 4.9 7.3 27.8 47.9 12.2 100.0
As shown in Table 4, the dominant religion is Roman Catholic with 86.1 percent. This is in congruence to the statistics in the Philippines which considers Roman Catholic as the dominant religion that is 85 percent of the population. In Cagayan de Oro City, Roman Catholic is comprised of 82.7 percent of the total population (National Statistical Coordination Board). A portion of this
percentage are from Barangay Camaman-an, as evidenced by presence of chapels in every sitio. Table 4: Distribution of Respondents According to Religion Religion Roman Catholic Islam Protestant Iglesia Ni Cristo Frequency 248 4 9 7 Percent 86.1 1.4 3.1 2.4
54
Seventh Day Adventist Others Total
6 14 288
2.1 4.9 100.0
Problem 2: What is the level of awareness on HIV-AIDS of the respondents in terms of: 2.1 Transmission; 2.2 Myths; and 2.3 Preventive Measures? In the level of awareness in terms of transmission of HIV-AIDS, Table 5 showed that respondents were moderately aware with an overall mean of 2.21 and a standard deviation of 0.80, which shows that the respondents responses were consistent. Specifically, they were highly aware that HIV can be transmitted through unprotected sex (70.5 percent), blood transfusion (67.4 percent) and sharing of needles (59 percent). This implies that the out-of-school youth in the area were highly aware about some of the common modes of transmission in acquiring HIV while moderately aware for some. The respondents were moderately aware that an infected mother can transmit the virus to her baby during pregnancy, delivery and breastfeeding, it is not transmitted by a mosquito bite and neither in touching infected people as well sharing the same utensils.
55
These findings were related to a study conducted by United Nations Economic and Social Commission for Asia and the Pacific (UNESCAP, 2009), which shows that many out-of-school youth believed that one could transmit HIV by touching an HIV infected person and through mosquito bites. Olujide (2011) affirmed that high proportion (82.1 percent) of their respondents were not aware of prevention of HIV-AIDS mother-to-child transmission. Another study of Kayode & Ogu (2011) supports the results by stating that those secondary school students in urban centers are very aware of safe blood transfusion, safe injection and the use of clean, sterilized piercing instruments as ways to prevent HIV transmission. Table 5: Level of Awareness among Respondents in HIV-AIDS Transmission Indicators of HIV transmission Sexual intercourse without using condom Receiving blood from an HIVinfected person Sharing the same needle or syringe with an HIV-infected person From HIV-infected mother to her baby during pregnancy, delivery or through breast feeding Mosquito bites Mean 2.55 2.50 2.35 SD 0.75 0.78 0.84 Interpretation Highly Aware Highly Aware Highly Aware
2.07 1.95
0.86 0.86
Moderately Aware Moderately Aware
56
Touching people infected with HIV Sharing the same utensils with an HIV-infected person Average
2.06 2.01 2.21
0.83 0.68 0.80
Moderately Aware Moderately Aware Moderately Aware
Table 6 presents the level of awareness on different myths on HIV-AIDS in which the respondents were moderately aware with an overall mean of 2.04 and a standard deviation of 0.75 which denotes that the respondents answers were homogeneous. Specifically, they were moderately aware that a person can get HIV from oral sex; that a woman can get HIV if she had sex during her period and that coughing and sneezing do not spread HIV. These suggest that respondents somehow believed on these myths. It is therefore possible that they will allow themselves to engage in risky sexual behaviors such as oral sex and having sex during menstrual period, which may increase the risk for HIV infection. This also implies that they may avoid those HIV infected persons with the belief that the virus can be transmitted through sneezing and coughing. However, the respondents were highly aware that people who have been infected with HIV dont quickly show serious signs of being infected, and that there is no existing vaccine that can
57
facilitate immunity to humans from acquiring HIV. With this awareness, they may have an increased sense of fear of getting HIVAIDS which may drive them to seek for consultation and undergo diagnostic tests for confirmation. These findings supports with that of Reich and Painter (1994), who revealed that some minority gay men believe that oral intercourse is safe. This perception may be significant determinants of their involvement in the practice of unsafe sex that pose either high risks for HIV infection. The Young Adult Fertility and Sexuality Survey (2003), a DOH national survey among young people on HIV and STI awareness, also shows that many (73 percent) thought that they are immune to HIV. Table 6: Level of Awareness of Respondents in HIV-AIDS Myths Indicators of HIV-AIDS myths People who have been infected with HIV quickly show serious signs of being infected There is a vaccine that can stop adults from getting HIV A person cannot get HIV from oral sex Coughing and sneezing spreads HIV A woman cannot get HIV if she had sex during her period Mean 2.43 2.38 1.74 1.83 1.84 SD 0.8 1 0.8 1 0.7 3 0.6 7 0.7 6 Interpretation Highly Aware Highly Aware Moderately Aware Moderately Aware Moderately Aware
58
Average
2.04
0.7 5
Moderately Aware
Table 7 presents the level of awareness on the preventive measures on HIV-AIDS in which the respondents were moderately aware with an overall mean of 1.96 and a standard deviation of 0.74 showing uniformity of the respondents answers. Moreover, the level of awareness on the preventive measures of HIV-AIDS revealed that the respondents were highly aware that washing oneself thoroughly (particularly ones private parts) after sex, cannot prevent HIV-AIDS transmission. This implies that the respondents perceived that perineal care alone, though it is an important hygiene practice, does not prevent the spread of HIV, thus they knew that it is not a preventive measure. However, respondents were moderately aware on most of the myths. This data implies that they may have a higher risk to acquire HIV since they werent highly aware in protecting themselves from HIV-AIDS. These results are the same with the study facilitated by UNESCAP (2009), which reveals that among the misperceptions, were persistent beliefs that good nutrition, exercise, personal hygiene and taking antibiotics could prevent HIV infection.
59
Table 7: Level of Awareness of Respondents on HIV-AIDS Preventive Measures Indicators of HIV-AIDS prevention Correct and consistent use of condoms whenever having sex Not sharing needles/syringes with others Not having sex Not by taking herbal medicines after having sex Not by take antibiotics before and after having sex Not by washing oneself thoroughly (particularly ones private parts) after sex Not by eating nutritious food Not by doing exercise regularly Average
Mean 1.87 2.22 2.01 1.90 1.77 2.34 1.74 1.81 1.96
SD 0.86 0.87 0.82 0.57 0.62 0.86 0.66 0.68 0.74
Interpretation Moderately Aware Moderately Aware Moderately Aware Moderately Aware Moderately Aware Highly Aware Moderately Aware Moderately Aware Moderately Aware
As presented in Table 8 showing the level of awareness on HIV-AIDS of the respondents, 74.7 percent were rated moderately aware, wherein they are categorized as having an average awareness but may be slightly misguided by a belief on a misconception. It is followed by 16.3 percent of the respondents, rated as unaware. This result is may be because the out-of-school
60
youth in the area have lesser exposure to authorized learning environment and more contact to unreliable information sources such as media, internet, neighbors and peers. They may share personal experiences, hearsays and wrong information among themselves. Supporting this result, Laguna (2004) said that majority (80 percent) have moderate knowledge regarding AIDS, from a study on Knowledge of HIV/AIDS and Unsafe Sex Practices among Filipino Youth. But on the contrary, the finding of this study is not in congruence to a survey conducted by the UNESCAP in 2009 to the out-of-school youth in China, Sri Lanka, China and including the Philippines which revealed that there is high awareness of HIV-AIDS among respondents. Table 8: Level of Awareness on HIV-AIDS of the Respondents Level of Awareness Frequency Highly aware 26 Moderately aware 215 Unaware 47 Total 288 Mean = 2.07 Std Deviation = 0.31 Percent 9.0 74.7 16.3 100.0
Problem 3: Is there a significant difference on the level of awareness of HIV-AIDS when grouped according to:
61
3.1 Age; 3.2 Gender; 3.3 Educational attainment; and 3.4 Religion? Table 9 presented that there is no significant difference on the respondents level of awareness on HIV-AIDS when grouped according to age. The t-stat of 0.896 is not significant to 0.05 level of significance therefore the null hypothesis is accepted. The finding implies that the level of awareness on HIV-AIDS between
adolescents and young adults were the same. It doesnt follow that as age increases, his level of awareness with regards to HIV-AIDS also increases. In line with the discoveries of Benedict (2001), Akpama (2007) and Omotosho (2004), adolescents and young adults with no formal sex education have common familiarity or perceptions on HIV-AIDS and its preventive measures. The results were similar to a study by Momoh (2007), which showed that the level of awareness on HIVAIDS between ages 16-25 years old and above is the same. On the other hand, it is contradicting to the study of Laguna (2004), which revealed that older adolescents (20-24) are more knowledgeable about AIDS than the younger ones (15-19).
62
Table 9: Differences on Level of Awareness on HIV-AIDS when Grouped According to Age Level of Awareness Moderately aware Moderately aware Test Statistic (p-value) 0.896 n
Age 15-19 20-24
Mean 2.0832 2.0508
SD .30576 .30614
(.371) Legend: n = not significant at 0.05 level of significance In Table 10, the respondents level of awareness on HIV-AIDS when grouped according to gender, have the U-stat of 9.893 which is not significant to 0.05 level of significance. Therefore the null hypothesis is accepted. Both genders have almost the same means thus they are both moderately aware. This finding is supported in a study entitled An Assessment of the Role of School Counselors in Preventing HIV-AIDS among Secondary School Students in Osun, State, Nigeria by Ajila, et al. (2012), who pointed out that there is no significant difference between male and female secondary school students practice of precautionary measures against the transmission of HIV-AIDS. However, Laguna (2004) revealed, there is a noticeable gender difference on the knowledge of sexually transmitted disease.
63
Table 10: Differences on Level of Awareness of HIV-AIDS when Grouped According to Gender Gender Male Female Mean 2.0657 2.0728 SD .28616 .33410 Interpretation Moderately aware Moderately aware Test Statistic (p-value)
9.893 n (.580) Legend: n = not significant at 0.05 level of significance As presented in Table 11, the respondents level of awareness on HIV-AIDS when grouped according to educational attainment, have the K-stat of 4.723 which is not significant to 0.05 level of significance. Therefore the null hypothesis is accepted. It is shown that respondents at all level of educational attainment were moderately aware. This implies that the out-of-school youths educational attainment does not contribute to their level of awareness. This may suggest that reproductive health and sex education in schools were either not taught by teachers or may not be effective. This may be because of the fear to corrupt the minds of the young and to their belief that parents are the key persons to talk about these sensitive matters. The result of this study contradicts the study of Laguna (2004) that education reinforces knowledge regarding HIV-AIDS. Moreover,
64
Momoh (2007) on his study concluded that the higher academic level of students, the more informed they are about HIV-AIDS. Table 11: Differences on Level of Awareness of HIV-AIDS when Grouped According to Educational Attainment
Educational Attainment Elementary level Elementary graduate High school level High school graduate College level Test Statistic (pvalue)
Mean 2.1607 2.0452 2.1138 2.0453 2.0343
SD .25584 .23287 .31179 .31402 .31196
Interpretation Moderately aware Moderately aware Moderately aware Moderately aware Moderately aware
4.723 n (.317)
Legend: n = not significant at 0.05 level of significance As presented in Table 12, the respondents level of awareness on HIV-AIDS when grouped according to religion, have the F-stat of
12.221 (p-value=0.032),
which is significant to 0.05 level of
significance. Therefore, the null hypothesis is rejected. It also shows the level of awareness when grouped according to religion which revealed that Islam religion is highly aware with the mean value of 2.3375 compared to the other religions which showed a lower mean value. The result shows that Islamic people are knowledgeable on their attitude towards sex because of their strict adherence to the doctrine that was taught to them.
65
This finding can be explained by the AIDS Education and Research Trust (2012), an international AIDS charity organization, which states that, Many people believed that it is inappropriate to talk to young people about sensitive subjects such as sex and drug abuse. They fear that doing so will encourage young people to indulge in risky behaviors. Such attitudes are often based on moral or religious views rather than evidence and severely limit HIV-AIDS education around the world. Table 12: Differences on Level of Awareness of HIV-AIDS when Grouped According to Religion
Religion Roman Catholic Islam Protestant Iglesia Ni Cristo Seventh Day Adventist Others Mean 2.0804 2.3375 2.0389 1.8571 1.9750 1.9464 SD .30912 .22867 .41592 .18127 .12550 .19948 Interpretation Moderately aware Highly aware Moderately aware Moderately aware Moderately aware Moderately aware 12.221* (.032) Test Statistic (pvalue)
Legend: * = significant to 0.05 level of significance CHAPTER 5 SUMMARY, CONCLUSION AND RECOMMENDATION
Summary of the Study
66
This study determined the Level of Awareness on HIV-AIDS among out-of-school youth ages 15-24 as of the year 2012, and who exclusively reside at Barangay Camaman-an, Cagayan de Oro City. The respondents of this study were 288, based on the Finite Population formula calculation on sample size. Snowball or
networking sampling method was used in the selection of the respondents. The study used a modified questionnaire in collecting data to assess the level of awareness among out-of-school youth. The test instrument was pre-tested and was proven valid and reliable (0.725 Cronbach alpha). Summary of Findings The following were the relevant findings drawn from the result of the study: 1. Majority of the respondents were from the adolescent group, ages 15-19 years old. More than half were male. In terms of Educational Attainment, majority of the
respondents are high school graduates. The dominant religion is Roman Catholic. 2. The level of awareness on HIV-AIDS among the
respondents, was rated moderately aware. Specifically, they were highly aware on transmission of
67
HIV through unprotected sex, blood transfusion and sharing of needles. They were moderately aware about
transmission from mother to child during pregnancy, delivery or through breast feeding. With regards to myths on HIV, they are moderately aware that a person can get HIV from oral sex, that a woman can get HIV if she had sex during her period and that coughing and sneezing do not spread HIV.
Nevertheless, the respondents were highly aware that people who have been infected with HIV dont quickly show serious signs of being infected, and there is no existing vaccine that can facilitate immunity to humans from acquiring HIV. Lastly, in terms of preventive measures, they were moderately aware on the use of condoms, abstinence and not sharing of needles. However, they were highly aware that perineal care alone does not prevent them from acquiring the disease. 3. The null hypothesis was tested and proven that there is no significant difference on level of awareness about HIV-AIDS
68
among the out-of-school youth when grouped according to age, gender and educational attainment. However, there is a significant difference in terms of religion. Conclusions Based on the findings of the study, the following can be concluded: Majority of the respondents ages 15-19 years old; this age group belongs to Secondary education where most of the respondents highest educational attainment as well. It is at this level where school drop-outs are common. Considering that they are already capable of working, thus they seek jobs to help their family rather than continue schooling. Males were more likely to be an out of school than females. They have a high tendency to be pulled out from school due to short term opportunities, peer pressure and threatening behaviors. The dominant religion is Roman Catholic, which is congruent to the statistics in the Philippines as well as in Cagayan de Oro City.
69
Overall, findings showed a moderate level of awareness on HIV-AIDS among out-of-school youth in Barangay Camamanan. Therefore, they are familiar about HIV-AIDS but their awareness in terms of transmission, myths and preventive measures, is insufficient and there are still misconceptions to correct.
The out-of-school youth in Barangay Camaman-an were susceptible in acquiring HIV-AIDS because of their moderately awareness. This may be due to lesser exposure to authorized learning environment and more contact to unreliable
information sources such as media, internet, neighbors and peers. They may share personal experiences, hearsays and wrong information among themselves, thus misguiding them about HIV-AIDS. The level of awareness of the out-of-school youth in Barangay Camaman-an on HIV-AIDS revealed no significant difference by age, gender, and educational attainment. This is because there was no formal sex education implemented even in schools which is evidenced by having the same moderate awareness among 15-24 years olds, both genders and in all
70
education levels. However, the results of the study revealed that religion plays a significant role in HIV-AIDS awareness since attitudes and behaviors regarding sex are often based on moral or religious views. Recommendations Based on the findings and conclusions, the following are recommended: 1. Department of Health and Barangay Health Center The results of our study will give them an idea that the out-ofschool youth in Barangay Camaman-an were moderately aware on HIV-AIDS. A campaign for the purpose of disseminating the results of this study will be channeled to the head of the local health center and DOH to assist and possibly bolster awareness among out-ofschool youth regarding HIV-AIDS prevention and transmission. They should appropriately address the concerns of this vulnerable group and strengthen clinical services for HIV-AIDS. If possible, screening of the high-risk groups such as the respondents of this study will be proposed as an important measure to identify infected persons and control the spread of the disease. Moreover, they should initiate health programs and projects in order to inform the out-of-school
71
youth
about
the
facts
regarding
HIV/AIDS
and
eliminate
misconceptions and myths. This can be done through micro teaching, distribution of pamphlets and posting of tarpaulins in different areas. This could be a means to increase the awareness of the out-of-school youth regarding the matter and help them refrain from doing risky behaviors. DOH should also provide adequate funding for HIV-AIDS research, preventive education, medical care, and support services. 2. Department of Education They should include in the school curriculum about
reproductive health emphasizing HIV-AIDS prevention. They should also facilitate in expanding the coverage of sex education to the outof-school youth and formulate and implement an innovative curriculum design and delivery systems to bring education to the youth who might not have access in-school opportunities. 3. Religious leaders It is recommended that they should emphasize in their religious teachings about their views, beliefs and the importance of moral decisions regarding sexual practices so as the youth to be guided by principles and values. By this, they will be encouraged to abstain from risk behaviors which may lead them to acquire
72
HIV/AIDS. They can provide individual counseling and offering emotional and spiritual support especially to the out-of-school youths in their community. They can also collaborate with the local health centers personnel to help in alleviating the incidence and spread of HIV/AIDS. 4. Xavier University-College of Nursing To the faculty and students, the results of our study should encourage them to propose and implement a social responsibility project about HIV/AIDS awareness regarding its prevention and transmission especially among the out of school youth. They can also provide health teachings, promoting reproductive health
education during their Community Health Nursing (CHN) activities. These actions will possibly aid in increasing the level of awareness of the citizens most especially among out-of-school youth and
empowering them to safeguard themselves against HIV-AIDS. 5. Parents As the primary responsible persons to their children, all parents should allot time for their children to talk about sex education and prevention of sexually transmitted diseases,
particularly HIV-AIDS. They should also be involved in programs and seminars which can provide them necessary information that will aid
73
them in teaching their children. As possible, they should support and encourage their children to attend school which provides a venue for health education. 6. Out-of-School Youth To all out-of-school youth, especially in Barangay Camaman-an, they should willingly cooperate and submit their selves in health programs and seminars regarding prevention of sexually-transmitted diseases, particularly HIV-AIDS. They should know that by being aware of its transmission and preventive measures, they would have a reduced chance to be infected. Moreover, they should be encouraged to continue schooling to keep them proactive and updated especially in terms of health promotion. 7. Future researchers They should do further research and investigation in
connection to this study. It is recommended to conduct the survey in a larger sample size, expanding the coverage to other barangays here in Cagayan de Oro City. Also, they can study other independent variables such as income, place of residence and exposure to media. They could also determine existing relationships, rather than differences. BIBLIOGRAPHY
74
A. Books Alcamo, E. (1997). AIDS: The biological basis. USA: Times Mirror Higher Education Group, Inc. Allender, J.A., Rector, C., and Warner, K.D. (2010). Community health nursing: Promoting and protecting the publics health. Philadelphia: Wolters Kluwer Health| Lippincott Williams & Wilkins. Black, J. and Hawks, H. (2005). Medical surgical nursing. USA: Elsevier Saunders. Crimp, D. (1989). AIDS: Cultural analysis, cultural activism. England: The MIT Press. Faro, S. and Soper, D.E. (2001). Infectious diseases in women. Philadelphia: W.B. Saunders Company. Franklin, N. et al, (1995). Children, families HIV/AIDS psychosocial and therapeutic issues. New York: The Guild Ford Press. Friedman, S.B. (1998). Comprehensive adolescent health care (2nd Ed.). St. Louis: Mosby-Year book, Inc. Gove, P.B. (Ed.). (1996). Websters comprehensive dictionary. Springfield, Massachusetts, USA: Merriam-Webster Inc.
75
Haugaard, J.J. (2001). Adolescence as a likely time for the development of problematic behaviors. Problematic behaviors during adolescence. Boston: McGraw Hill Companies, Inc. Josselyn, I.M. (1971). Adolescence. New York: Harper & Row, Publishers. Kozier, B., et al. (2008). Fundamental of nursing concepts, process and practice. Singapore: Pearson Education, Inc. LeVay, S. (2006). Human sexuality. USA: Sinauer Associates. Lu, Y. & Essex, M. (2004), Aids in Asia. USA: Kluwer Academic/Plenum Publishers Malti-Douglas, F. (2007). Encyclopedia of sex and gender (Volume 1). Detroit: Gale Group. Muss, R. and Poston, H. (1998). Adolescent behavior and society. USA: The McGraw-Hill Companies,Inc. Papalia, D.E. (2006). A childs world: Infancy through adolescence. New York: Mc-Graw Hill Companies. Polit, D. and Hungler, B (1993). Essentials of nursing research: Methods appraisal and utilization. Philadelphia: J.B. Lippincott Company.
76
Rathus, S.A. (2008). Childhood and adolescence: Voyages in development. Canada: Thomson Wadsworth Corporation. Rathus, S.A. (2008). Human sexuality in a world of diversity. Boston: Pearson Education, Inc. Santrock, J.W. (2000). At risk youth. Psychology (6th Ed.). Boston: McGraw-Hill Companies, Inc. Seigel, L.J. et al. (2006). Juvenile deliquency (9th ed.). Thomson Wadsworth: USA. Stine, G.J. (2002).AIDS update 2002. New Jersey: Prentice Hall, Inc. B. Unpublished Materials Asinero, J.A. et al. (October, 2008). Level of awareness of female commercial sex workers in Cagayan de Oro City on STD and its preventive measures. Cabusas, C.G. (October, 2000). The level of awareness on RTI: A comparison between two groups of women in Cagayan de Oro City and Misamis Oriental, Philippines. Population Education A dimension of youth development programs population center foundation. Makati Phil., 1977 C. Periodicals and Journals
77
Leung-Chen, P. (2008). Syphilis makes another comeback. American Journal of Nursing. Vol. 108, No. 2, p.28 NorMin ranks 4th with high number of OSY. (November 9, 2011). SunStar Cagayan de Oro, 16, 2. Wallace, M. (2008). Assesssment of sexual health in older adults. American Journal of Nursing. Vol. 108, No.7. p.54 D. Electric Journals Burns, A.A. (2004). Reaching out of school youth with reproductive health and HIV/AIDS information and services. Retrieved January 5, 2012, from www/phi.org/youthnet Ajila, M.A.(2009). An assessment of the role of school Counselors in preventing Retrieved HIV/AIDS among 23, secondary 2012, school from students. http:// September
http://www.bangladeshsociology.org/An%20Assessment%20of %20the%20Role%20of%20School%20Counsellors%20in %20Preventing%20HIV.pdf Akpama, E.G.(2012).Adolescents perception and attitude to HIV/AIDS prevention among students. Retrieved September 23, 2012, from http:// http://cprenet.com/uploads/archive/UJMSS_121162.pdf Barrowman, C., et al (2001).Health risks among early school leavers:
78
Findings from an Australian study examining the reasons for, and consequences of, early school dropout. Health Education. Retrieved January 6, 2012, from http://proquest.umi.com/ pqdweb?did=119046860&sid=5&Fmt=3&clientld=43005& RQT=309&VName=PQD Bonnesma. O.(2012). Philippines. Raising of awareness on HIV/ AIDS in the from September 1, 2012 from
Retrieved
http://www.worldschool.nl/uploads/publications/348a05606ffaf 0c07b36dc0ba7d7ca53.pdf Burns, A.A. (2004). Reaching out of school youth with reproductive health and HIV/AIDS information and services. Retrieved January 5, 2012, from www/phi.org/youthnet Cabaraban, M.C., & Linog, M.T.S.C. (n.d.). Reproductive health and risk behaviors of adolescents in Northern 18, Mindanao, from Philippines. Retrieved February 2012,
http://www.childprotection. org.ph/monthlyfeatures/may2k6b.pdf Hartung, T.K.(2002). Aids awareness and Sexual Behavior in high HIV prevalence area. Retrieved September 23, 2012, from http.:// http://ijsa.rsmjournals.com/content/13/12/829.short Kayode A. (2011). School Location And Secondary School Students Awareness Of Human Immuno-Deficiency Virus/Acquired
79
Immune Deficiency Syndrome. Retrieved September 23, 2012, from http:// http://www.mcser.org/images/stories/JESR-SpecialIssues/JESR-September/adelakun%20kayode%20%20malachy % 20%20n. %20ogu.pdf Korra, A.(1997).Sexual 2012, from behavior and level of awareness on
reproductive health among youths. Retrieved September 23, http:// http://ejhd.uib.no/ejhd-v13/ejhd-v13-n2107.htm Laguna, E.P. (2004). Knowledge of HIV/AIDS and unsafe sex practices among Filipino youth. Retrieved February 18, 2012, from http:// paa2004.princeton.edu/download.asp? submissionId=42109 Lee. R. (2000). Male sexual risk behavior and HIV/AIDS: a survey in 3 Philippine cities. Retrieved from September 1, 2012 from http://www.fhi360.org/NR/rdonlyres/eom7gf7rarfd6m5r4wtotflc nbfejjbsvrzvdwyh7ynwul4tcijjer43ju7gaejzi5iypbp4t3g7xh/MEN NSAFinalreport.pdf Mehta, S. (n.d.). Perspectives for adolescent reproductive health in ESCAP region. Retrieved February 14, 2012, from http://www.unescap. org/esid/psis/po pulation/icpd/sec7.asp Murtala. M. R (2009). Knowledge and awareness of HIV/AIDS among
80
senior secondary students. Retrieved September 2, 2012 from http://www.ajol.info/index.php/bajopas/article/viewFile/63798/5 1618 Solomon, M.(2007). Women and HIV aids epidemic. Retrieved September 23, 2012, from http://www.freepatentsonline.com/ article/College-Student-Journal/169306814.html Perspective on language and literacy. (2009). Retrieved January 5, 2012, from http://proquest.umi.com E.Internet Castillo, J.J. (2009). Snowball sampling. Retrieved February 16, 2012, from http://www.experimentresources.com/snowballsampling.html#ix zz1mqdcUINx Chan, C. (September, 2005). Perils of generation sex. Retrieved February 18, 2012, from http://pcij.org/stories/perils-ofgeneration-sex/ Crisostomo S. (2012). 268 HIV cases last month. Retrieved from June 24, 2012 from http://www.philstar.com/Article.aspx? articleId=769159 &publicationSubCategoryId=63 Department of Health. Adolescent and youth health program (AYHP). (n.d.). Retrieved February 13, 2012, from http://www.doh.gov.ph/ node/338
81
HIV Cases Rise To Record-High. Retrieved June 25, 2012 from http://www.mb.com.ph/ National Statistics Office. (n.d.). 2010 Annual poverty indicators survey. Retrieved January 8, 2012, from http://www.census.gov.ph/data/ quickstat/region10/qs10051109.pdf NSO report on out-of-school-youth. (2004). Retrieved January 6, 2012, from http://www.childhope.org.ph/unesco.php? subaction=show full&id=1099970424&archive=&start_from=&ucat=1&v Philippines struggles with AIDS (December 2011). Retrieved June 25,2012, philippines-struggles-aids Sexually Transmitted Diseases and HIV/AIDShttp://web.unfpa.org/ icpd/icpd5/meetings/ny_adolescent/reports/adoles.htm# Sheridan K. (2012) US experts urge approval of first AIDS prevention pill retrieved from June 24, 2012 from http://www.abscbnnews.com/lifestyle/05/11/12/us-experts-urge-approval-firstaids-prevention-pill from http://www.abscbnnews.com/lifestyle/12/03/11/
82
Valbuena J.(2009). Understanding the risk and vulnerabilities to HIV/AIDS of Filipino out of school youth. Retrieved September 2, 2012 from http://iussp2009.princeton.edu/papers/90687 Valmero, A. (May 2, 2012) . Bill seeks to curb AIDs as 10 new Pinoys get HIV daily. Retrieved June 25, 2012 from http://www.pnac.org.ph/index.php?mact=News %2Ccntnt01%2Cdetail %2C0&cntnt01articleid=389&cntnt01origid=39&cntnt01return id=39 F. Other Documents Cagayan de Oro City Hall. Information department. (December, 2011) Department of Education. Comparative dropout rate in public secondary schools (2011). Camaman-an National Highschool. Performance Indicators: Enrollment (2011)
APPENDIX A LETTER OF PERMISSION FOR THE BARANGAY CHAIRMAN
83
APPENDIX B LETTER OF REQUEST FOR INFORMATION February 20, 2012 Dr. Jerie P. Calingasan
84
City Health Officer Cagayan de Oro City Dr. Jerie P. Calingasan, We, the 3rd year level nursing students of Xavier University Ateneo de Cagayan are currently having our research proposal for our Nursing Research (N40.1) regarding the level of awareness on HIV/AIDS among out-of-school youth in Cagayan de Oro city. In line with this, we would like to ask from your good office a statistics and prevalence of HIV/AIDS cases in each barangay in the city, entire Misamis Oriental, entire Mindanao and if possible any other data that would provide us with more information regarding the matter. We will determine the respondents of our research from the barangay with the highest prevalence of HIV/AIDS cases. The outcome of this research project will greatly have a positive impact for the knowledge and health of out-of-school youth and other people in the society. We truly acknowledge your positive response regarding this request. Thank you and God bless you! Respectfully yours, Lea Serrano BSN 3 Team Leader Noted by: Ms. Roselyn L. Bausing, RN, MAN Research Adviser, College of Nursing Xavier University Ateneo de Cagayan APPENDIX C CONSENT FORM (ENGLISH) In signing this document, I am giving my consent to participate in the research study about Level of Awareness on HIV-AIDS among Out-of School Youth.
85
Please Check the Box I confirm that I have read and understand the information sheet for the above study and have had the opportunity to ask questions. I understand that my participation is voluntary and that I am free to withdraw at any time, without giving reason. I agree to take part in the above study.
Name of Participant
Date
Signature
______________________ _________________
___________________
Maria Lea Serrano Research Leader
APPENDIX D CONSENT FORM (VISAYAN) Sa pagpirma aning dokumentoha, mitugot ako nga magsalmot aning pagtulon-an mahitungod sa Level of Awareness on HIV-AIDS among Out-of-school youth
86
Palihug i-check ang kahon Gicompirmar nako na nakabasa ug nakasabot ko sa mga impormasyon mahitungod ani na pagtulon-an ug naa koy katungod na mangutana. Nakasabot ko nga ang akong patisipasyon kay boluntaryo ug pwede nako i-undang bisan unsa na oras miskin walay rason. Mouyon ko na magpartisipar ani na pagtulon-an. Petsa Pirma _________________
Pangalan sa partisipante ______________________ Maria Lea Serrano Research Leader
___________________
APPENDIX E QUESTIONNAIRE (ENGLISH)
Xavier University College of Nursing Level of Awareness on HIV-AIDS among Out-of-School Youth Dear Respondents, We, the students of the College of Nursing, Xavier University would like to ask for your full cooperation in answering our survey questionnaire which pertains our study Level of awareness on HIV-AIDS among out-of-
87
school youth in Brgy. Camaman-an, Cagayan de Oro City in the year 2012. Rest assured that pertinent data/information written here will be strictly confidential. Thank you. LEVEL OF AWARENESS ON HIV/AIDS Part 1 - Profile of Respondents: 1. Name: (optional) ____________________________________ 2. Age: _________ 3. Gender: ( ) Male ( ) Female 4. Educational Attainment: Please put a check () mark on a given option below ( ) Elementary level ( ) Elementary Graduate ( ) High School level ( ) High School Graduate ( ) College level 5. Religious Affiliation: (Please check) ( ) Roman Catholic ( ) Muslim ( ) Protestant ( ) Iglesia ni Cristo ( ) Seventh Day Adventist ( ) Others (please specify) ______________ Part 2- Level of Awareness of HIV/AIDS 1. Please read each item carefully and decide honestly to what extent you have knowledge about HIV/AID in every item given. 2. Do not leave any item unanswered 3. Give each item a rating by putting a check ( ) mark.
88
Do you agree HIV can be transmitted through the following means 1. Mosquito bites 2. Touching people infected with HIV 3. From HIV-infected mother to her baby during pregnancy, delivery or through breast feeding 4. Sexual intercourse without using condom 5. Sharing the same utensils with an HIVinfected person 6. Receiving person blood from an HIV-infected
Agre e
Disagr ee
Not sure
7. Sharing the same needle or syringe with an HIV-infected person
Do you agree HIV transmission can be prevented through the following means 8. Eat nutritious food 9. Do exercise regularly 10. Correct and consistent use of condoms whenever having sex 11. Do not share needles/syringes with others 12. Do not have sex
Agre e
Disagre Not e sure
89
13.
Take herbal medicines after having sex
14. Take antibiotics before and after having sex 15. Wash oneself thoroughly (particularly ones private parts) after sex
Do you agree with the following HIVrelated statements 16. People who have been infected with HIV quickly show serious signs of being infected 17. There is a vaccine that can stop adults from getting HIV 18. A woman cannot get HIV if she had sex during her period 19. A person can get HIV from oral sex
Agre e
Disagre e
Not sur e
20. Coughing and sneezing do not spread HIV
APPENDIX F QUESTIONNAIRE (VISAYAN) Xavier University College of Nursing Level of Awareness on HIV-AIDS among Out-of-School Youth in Brgy. Camaman-an, Cagayan De Oro City in the Year 2012
90
Sa Manunubag, Kami ang mga istudyante sa College of Nursing gikan sa Xavier University nanghangyo sa inyong kooperasyon sa pagtubag sa among mga pangutana mahitungod sa among ginatun-an na Level of awareness on HIV-AIDS among out-of-school youth. Ang mga impormasyon ug datos nga inyong isulat dinhi, gikonsidera nga pribado ug konpidensyal. Daghang Salamat. LEVEL OF AWARENESS ON HIV/AIDS Part 1 Manunubag: 1. Pangalan: (kung pwede) ____________________________________ 2. Edad: _________ 3. Sekswalidad: ( ) Lalaki ( ) Babae 4. Nahuman sa Pag-eskwela: Palihug butang ug tsek () sa pilian ( ) Wala nakahuman sa elementarya ( ) Nakahuman ug elementarya (nigradweyt ug grade 6) ( ) Wala nakahuman sa hayskul ( ) Nakahuman sa hayskul (nigradweyt ug 4th year hayskul) ( ) Wala nakahuman ug college/ vocational 5. Relihiyon: (Palihug tsek) ( ) Romano Katoliko ( ) Islam ( ) Protestante ( ) Iglesia ni Kristo ( ) Sabadista ( ) uban pa: (palihug isulat)___________________ Part 21. Pagmabinantayon sa pagbasa kada parte ug pagmatinud-anon sumala
91
sa imong nahibaloan mahitungod sa HIV/AIDS. 2. Ayaw bilini nga blanko o walay tubag. 3. Gradohi kada usa ka bahin pinaagi sa pagbutang ug tsek ( ).
Mo-uyon ka ba nga ang HIV makuha pinaagi sa: 1. Paak sa lamok 2. Paghikap sa taong adunay HIV 3. Gikan sa inahan nga adunay HIV ngadto sa anak sa panahon sa pagburos, pagpanganak, ug pagpasuso 4. PagJerjer o pagpakighilawas nga walay gamit nga condom 5. Pakigsalo sa parehong galamiton sama sa kutsara ug tinidor sa taong adunay HIV 6. Pagdawat sa gi-abuno nga dugo gikan sa tao nga adunay HIV 7. Pakigsalo ug gamit sa dagum o indyeksyon
Uyon
Supak
Dili Sigurado
Mo-uyon ka ba nga ang pagpasa sa HIV kay malikayan pinaagi sa: 8. Pagkaon ug masustansyang pagkaon 9. Regular nga ehersisyo 10. Insakto ug kanunay nga paggamit ug condom kung makighilawas o magjerjer 11. Dili pag-gamit sa dagom o indyeksyon nga gigamit na sa uban. 12. Dili makighilawas o magjerjer
Uyon
Supa k
Dili Sigurad o
92
13. Pag-inom ug mga herbal nga tambal inig-kahuman magjerjer o pakighilawas 14. Pag-inom ug antibiotic sa dili pa ug paghuman magjerjer o makighilawas 15. Paghugas ug tarong sa kinatao paghuman ug jerjer o makighilawas Uyon Supak Dili Sigurado
Mi-uyon ka ba niining mga istorya2x bahin sa HIV nga: 16. Ang taong nataptan sa HIV kay makasinati dayon sa mga seryosong simtomas. 17. Adunay bakuna nga makapugong sa mga tao sa pagkuha sa HIV. 18. Kung makighilawas o magjerjer ang babae nga gidugo, dili siya matakdan ug HIV. 19. Makuha sa tao ang HIV pinaagi sa pakighilawas o magjerjer gamit ang baba ngadto sa kinatawo. 20. Ang pag-ubo ug pangatsi kay dili makatakod sa HIV. APPENDIX G
SAMPLE SIZE COMPUTATION Using the Finite Population Formula: n= Nz2 [p (1-p)] Nd2 + z2 [p(1-p)]
93
N= approximately 1,142 z = 1.96 p = .50 d = .05
n= (1142)(1.962) [0.5 (1-0.5)] (1142)(.052) + (1.962) [0.5 (1-0.5)] n= (1142)(3.8416) [0.25] (1142)(0.0025) + (3.8416) [0.25] n=288 respondents as sample size
APPENDIX H STATISTICAL FORMULA 1. Frequency and Percentage The formula used in the application of this technique is: % = (f/n) x 100 where: % = percentage f = frequency n = number of cases or total sample
94
2. Simple/ Arithmetic Mean Formulas: Where: x=x/n x= mean x = value/ sum of all the given elements n= total number of elements 3. Standard Deviation
4. T- Test Formula:
Where:
4. F-Test (ANOVA) Formula: F= sa2/s32
95
Where:
F= F-test result sa2= variance of the first group s32= variance of the second group
3. Mann-Whitney test
Rank the combined set of data from the two groups from lowest to highest with tied scores receiving a rank equal to the average position of those scores in the ordered array (see the example). Compute
Where:
U is the Mann-Whitney statistic, N1 and N2 are the number of cases in samples 1 and 2, respectively R1 is the sum of the ranks for the first sample. 4. Kruskal-Wallis test
96
Where: is the number of observations in group is the rank (among all observations) of observation from group is the total number of observations across all groups , is the average of all the .
6.
Post Hoc Analysis using LSD
The least significant difference between two means is calculated by:
(least significant difference) procedure
LSD = t
Where:
2MSE / n*
t is the critical tabled value of the t-distribution with the df associated with MSE, the 2 denominator of the F statistic n* is the number of scores used to calculate the means of critical interest. APPENDIX I DATA GATHERING DOCUMENTATION
Researchers Barangay Camaman-an Researchers going to different sitios of introducing themselves and asking permission to the out-of-school youth to be a respondent
97
Respondents were asked to sign the consent form.
Reinforcing the instructions and encouraging them to ask any clarifications about the questionnaire.
98
The respondents are answering the survey questionnaires.
99
Asking for any referrals and locating other out-of-school youth
CURRICULUM VITAE
100
Name: Maria Lea Serrano Personal Data Place of Birth Date of Birth Address Balulang, Cagayan de Oro City August 6, 1991 021 Lapasan, Cagayan de Oro, City Civil Status Parents Single Mr. Leandro Serrano & Mrs. Susie Serrano
Siblings Michael, Rafael, Angela,
Western
Kolambog,
Gabriel, Augustine, John Paul Cell Phone Number Email Address 09263705053 wisdomleyh@yahoo.com
101
Name: Melody Kaye A. Monsanto Personal Data Place of Birth Date of Birth Address Malaybalay City May 27, 1993 Block 2 Lot 4&6 Villa de Azura Subdivision, Malaybalay City Civil Status Parents Single Atty. Hollis C. Monsanto & Mrs. Honeylit A. Monsanto Siblings Cell Phone Number Email Address melody_kaye272000@yahoo.com Matthew Kressler A. Monsanto 09177150056/09321910365 Casisang,
102
Name: Ruth Ann O. Rentuma Personal Data Place of Birth Date of Birth Address Talisayan, Misamis Oriental April 1, 1993 Block 4 lot 4 Gemelina St. Virginia Homes, Iponan, Cagayan de Oro City Civil Status Parents Single Mr. Rolando A. Rentuma & Mrs. Tessie O. Rentuma Cell Phone Number Email Address 09154507731 rentumaruthann@yahoo.com
103
Name: Cristina G. Malicse Personal Data Place of Birth Date of Birth Address Cagayan De Oro City April 6, 1990 298 Zone 1 Kauswagan, Cagayan De Oro City Civil Status Parents Single Mr. Paulino A. Malicse, Jr. & Mrs. Eva G. Malicse Sibling Cell Phone Number Email Address Bryan Joseph G. Malicse 09352537023 seiclam_4690@yahoo.com
Name: Jillben Rey O.
Tabanao
104
Personal Data Place of Birth Date of Birth Address Civil Status Parents Lianga Surigao del Sur March 6, 1991 Lianga Surigao del Sur Single Mr. Bernabe O. Tabanao & Mrs. Marlita O. Tabanao Siblings Cell Phone Number Email Address Joann, Jestoni, John, Rafael 09272852985 jillbenreytabanao@yahoo.com
Name: Jica Nicole V. Parchamento Personal Data
105
Place of Birth Date of Birth Address
Malaybalay City, Bukidnon August 17, 1992 Helens Dormitory, DoloresNavarro St., Cagayan de Oro City
Civil Status Parents
Single Mr. Renee J. Parchamento & Mrs. Daisy V. Parchamento
Siblings Cell Phone Number Email address
Kim Joshua Parchamento 09177960817 jicaparchamento@yahoo.com
Name: Demelyn Ann J. Pagute Personal Data Place of Birth Date of Birth Cagayan de Oro City August 25, 1991
106
Address
Zone 6 VSC Kareteras Bon-bon Cagayan de Oro City
Civil Status Parents
Single Mr. Demetrio L. Pagute & Mrs. Jocelyn J. Pagute
Siblings
Julie Rose J. Pagute & Precious Kyle Vanice J. Pagute
Cell Phone Number Email Address
09061023638 demie25_xuhs@yahoo.com
Name: Raphael Russ M. Pasimio Personal Data Place of Birth Cagayan de Oro City
107
Date of Birth Address
March 23 1992 Agape Drive Tibasak Macasandig De Oro City Cagayan
Civil Status Parents
Single Mr. Rolando V. Pasimio Sr. & Mrs. Rosie Linda M. Pasimio
Siblings
Rolando Pasimio Jr. & Rosario Lei Pasimio
Cell Phone Number Email Address
09156634970 Raphael_russ @yahoo.com
Name: Kate Johanna O. Naranjo Personal Data
108
Place of Birth Date of Birth Address
Gingoog City December 1, 1992 J. Cuerdo St. Barangay. 24-A Gingoog City
Civil Status Parents
Single Mr. Saulo S. Naranjo & Mrs. Nancy O. Naranjo
Siblings
Justin Paolo O. Naranjo & Johann Philip O. Naranjo
Cell Phone Number Email Address
09265035237 annahoj_yenoh@yahoo.com
Vous aimerez peut-être aussi
- Allen College of Homoeopathy: PhosphorusDocument4 pagesAllen College of Homoeopathy: PhosphorusMuhammad Ata Ul MustafaPas encore d'évaluation
- IMCIDocument27 pagesIMCImesdejen100% (6)
- Alteration in Inflammatory and Immunologic Response 2012Document22 pagesAlteration in Inflammatory and Immunologic Response 2012Pamela BagabaldoPas encore d'évaluation
- Insecticidal Activity of Lemongrass Oil As Mosquito Repellent PerfumeDocument36 pagesInsecticidal Activity of Lemongrass Oil As Mosquito Repellent PerfumeKristan RialaPas encore d'évaluation
- Level of Awareness and Attitude of Grade 12 GAS Students On Selected Sexually Transmitted Diseases Quantitative Research ProposalDocument37 pagesLevel of Awareness and Attitude of Grade 12 GAS Students On Selected Sexually Transmitted Diseases Quantitative Research ProposalCharlz HizonPas encore d'évaluation
- Impetigo: A Bacterial Skin InfectionDocument13 pagesImpetigo: A Bacterial Skin InfectionTasya SyafhiraPas encore d'évaluation
- Chapter 2Document6 pagesChapter 2Nica Jane MacapinigPas encore d'évaluation
- Pengenalan Icd-10 Struktur & IsiDocument16 pagesPengenalan Icd-10 Struktur & IsirsudpwslampungPas encore d'évaluation
- Social Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsD'EverandSocial Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsPas encore d'évaluation
- Face To Face ClassesDocument1 pageFace To Face ClassesRalen Beronilla Odchigue100% (1)
- IntussusceptionDocument60 pagesIntussusceptionAhmad Abu KushPas encore d'évaluation
- HIV/AIDS Awareness Evaluation in The Junior and Senior High School Students of University of The East Caloocan (UEC)Document11 pagesHIV/AIDS Awareness Evaluation in The Junior and Senior High School Students of University of The East Caloocan (UEC)Sebastian Miguel CarlosPas encore d'évaluation
- Hiv Aids Thesis TopicsDocument5 pagesHiv Aids Thesis TopicsCollegePapersHelpSingapore100% (1)
- 3574-Article Text-80905-1-10-20220927Document8 pages3574-Article Text-80905-1-10-20220927Assuming AssumingxdPas encore d'évaluation
- Among Youth: Hiv/AidsDocument5 pagesAmong Youth: Hiv/AidsShahnaz RizkaPas encore d'évaluation
- Final Papers QuantitativeDocument95 pagesFinal Papers QuantitativeDahl xxPas encore d'évaluation
- The Problem and Its ScopeDocument26 pagesThe Problem and Its ScopeBryantPas encore d'évaluation
- Awareness and Knowledge of Secondary School Students Towards Sexually Transmitted InfectionsDocument58 pagesAwareness and Knowledge of Secondary School Students Towards Sexually Transmitted InfectionsSolomonPas encore d'évaluation
- Lived Experiences of Individuals With Sexually Transmitted Infections (STIs) : An Input To Infectious Disease Awareness and PreventionDocument12 pagesLived Experiences of Individuals With Sexually Transmitted Infections (STIs) : An Input To Infectious Disease Awareness and PreventionPsychology and Education: A Multidisciplinary JournalPas encore d'évaluation
- Importance of Knowledge about Prevention of Sexually Transmitted DiseasesDocument24 pagesImportance of Knowledge about Prevention of Sexually Transmitted DiseasesLorraine ZaratePas encore d'évaluation
- Saturday Group - Level of Knowledge On HIV AIDS Among Adolescents in Selected Barangays in Malapatan - LatestDocument77 pagesSaturday Group - Level of Knowledge On HIV AIDS Among Adolescents in Selected Barangays in Malapatan - Latestromie_galloPas encore d'évaluation
- Christine Jean Ceridon-1 FINAL (Autosaved) - 1Document40 pagesChristine Jean Ceridon-1 FINAL (Autosaved) - 1Christine Jean CeredonPas encore d'évaluation
- Aids Research Paper ConclusionDocument6 pagesAids Research Paper Conclusionjmforlwgf100% (1)
- Hiv Prevention Literature ReviewDocument9 pagesHiv Prevention Literature Reviewafmzatvuipwdal100% (1)
- Research Paper On Aids PDFDocument5 pagesResearch Paper On Aids PDFm1dyhuh1jud2100% (1)
- Awareness of HIV/AIDS Among Grade 10 Students in Teofilo V. Fernandez National High SchoolDocument18 pagesAwareness of HIV/AIDS Among Grade 10 Students in Teofilo V. Fernandez National High SchoolChristine Jean CeredonPas encore d'évaluation
- Literature Review Hiv AidsDocument7 pagesLiterature Review Hiv Aidsfvga1ym2100% (1)
- 241-246-Malleshappadoc.100230516 ImpDocument6 pages241-246-Malleshappadoc.100230516 ImpSunny OberaiPas encore d'évaluation
- Example of Research Paper About HivDocument6 pagesExample of Research Paper About Hivc9qb8gy7100% (3)
- Research Paper Topics About HivDocument8 pagesResearch Paper Topics About Hivlrqylwznd100% (1)
- Suji. Y. I Year M.Sc. Nursing Masood College of Nursing Bikarnakatta, Kulshekar Post, MANGALORE-575005Document15 pagesSuji. Y. I Year M.Sc. Nursing Masood College of Nursing Bikarnakatta, Kulshekar Post, MANGALORE-575005pavinPas encore d'évaluation
- HIVAIDS-related Knowledge and Behavior Among School-AttendingDocument11 pagesHIVAIDS-related Knowledge and Behavior Among School-Attendingcarmen lopezPas encore d'évaluation
- 10 - Dwiti Hikmah Sari - 16ik466Document11 pages10 - Dwiti Hikmah Sari - 16ik466titi hikmahsariPas encore d'évaluation
- Program Plan Final AssignmentDocument20 pagesProgram Plan Final Assignmentapi-505655836Pas encore d'évaluation
- Fullpaper Huriati Sitgma HIVAIDSDocument4 pagesFullpaper Huriati Sitgma HIVAIDSmaria ulfahPas encore d'évaluation
- The Importance of Sex Education Among The YouthDocument23 pagesThe Importance of Sex Education Among The YouthPatricia Kate DominguezPas encore d'évaluation
- The Impact of Perinatal HIV Infection On Older School-Aged Children's and Adolescents' Receptive Language and Word Recognition SkillsDocument9 pagesThe Impact of Perinatal HIV Infection On Older School-Aged Children's and Adolescents' Receptive Language and Word Recognition SkillsAndrew MoriartyPas encore d'évaluation
- Research Paper Outline On Hiv AidsDocument4 pagesResearch Paper Outline On Hiv Aidsc9rz4vrm100% (1)
- Human Immunodeficiency Virus Awareness of The Adolescent Students in Tomas Del Rosario CollegeDocument49 pagesHuman Immunodeficiency Virus Awareness of The Adolescent Students in Tomas Del Rosario CollegePherlyn MarceloPas encore d'évaluation
- Major Paper Stigma Against People Living With Hiv/AidsDocument17 pagesMajor Paper Stigma Against People Living With Hiv/AidsmusamuwagaPas encore d'évaluation
- Aids Research Paper ThesisDocument7 pagesAids Research Paper Thesisnatashajohnsonmanchester100% (2)
- Lorms Health and DiseasesDocument3 pagesLorms Health and Diseasessarahsze6Pas encore d'évaluation
- Research Paper On Aids in AmericaDocument6 pagesResearch Paper On Aids in Americajssoulznd100% (1)
- Hiv Related Thesis TopicsDocument4 pagesHiv Related Thesis TopicsHelpWritingPapersSalem100% (2)
- Research Paper On Hiv Aids PDFDocument6 pagesResearch Paper On Hiv Aids PDFafnhbijlzdufjj100% (1)
- Sexual Education FLCD 135Document7 pagesSexual Education FLCD 135Micah YapPas encore d'évaluation
- Assessment of Hiv/aids Awareness Program On The Prevalence of Hiv/aids Amongst Youths in Jos MetropolisDocument51 pagesAssessment of Hiv/aids Awareness Program On The Prevalence of Hiv/aids Amongst Youths in Jos MetropolisEbuka ChukwuemekaPas encore d'évaluation
- Example of Research Paper About AidsDocument7 pagesExample of Research Paper About Aidsgvym06g6100% (1)
- Hiv Prevention DissertationDocument8 pagesHiv Prevention DissertationCustomPaperSeattle100% (1)
- Nasarawa State College of Health Science and Technology, KeffiDocument6 pagesNasarawa State College of Health Science and Technology, KeffiMisbahudeen AbubakarPas encore d'évaluation
- Artikel-Hiv-Ayu NingrumDocument7 pagesArtikel-Hiv-Ayu NingrumAyu NingrumPas encore d'évaluation
- HIV/AIDS Determinants and Control FactorsDocument4 pagesHIV/AIDS Determinants and Control FactorsahiPas encore d'évaluation
- PLHIV Chapter 1 4 CompleteDocument186 pagesPLHIV Chapter 1 4 CompleteAngie Bucio MiraPas encore d'évaluation
- Rates and barriers of HIV status disclosure among women in developing countriesDocument9 pagesRates and barriers of HIV status disclosure among women in developing countriesTinkhaniMbichilaPas encore d'évaluation
- Literature Review On Hiv InfectionDocument7 pagesLiterature Review On Hiv Infectionafdtunqho100% (1)
- Blocking The Benefit of Group Based HIV Prevention Efforts During Adolescence - StigmaDocument8 pagesBlocking The Benefit of Group Based HIV Prevention Efforts During Adolescence - StigmaAMALIA PEBRIYANTIPas encore d'évaluation
- Comm 2700 PosterDocument4 pagesComm 2700 Posterapi-297174492Pas encore d'évaluation
- Research TopicDocument6 pagesResearch TopicJasmine Claire QuejarroPas encore d'évaluation
- HIV Among Youth: The NumbersDocument2 pagesHIV Among Youth: The NumbersJoseph RichardsonPas encore d'évaluation
- HIV/AIDS Research Papers from World Bank 2008-2009Document5 pagesHIV/AIDS Research Papers from World Bank 2008-2009Sneha NagvekarPas encore d'évaluation
- Research Paper AidsDocument4 pagesResearch Paper Aidsc9hpjcb3100% (1)
- Advocacy DraftDocument3 pagesAdvocacy DraftEUGENE DEUS GAVRIEL FAJARDOPas encore d'évaluation
- SdarticleDocument8 pagesSdarticlehafid nugrohoPas encore d'évaluation
- STUDENT KAP ON HIV/AIDSDocument22 pagesSTUDENT KAP ON HIV/AIDSbegosewPas encore d'évaluation
- Debate Communication - Pro Sex Education in Schools RESOLUTION: Lessons About Sexuality and Relationships Should Be Compulsory in SchoolsDocument4 pagesDebate Communication - Pro Sex Education in Schools RESOLUTION: Lessons About Sexuality and Relationships Should Be Compulsory in SchoolsAlexandra AlupeiPas encore d'évaluation
- Level of Awareness of STII SHS Students towards HIV/AIDSDocument17 pagesLevel of Awareness of STII SHS Students towards HIV/AIDSLanelyn TabiguePas encore d'évaluation
- Essay - Public HealthDocument15 pagesEssay - Public Healthtooba ShehzadPas encore d'évaluation
- Acknowledgement, Intro, Profile, Directory, Economic ProposalDocument34 pagesAcknowledgement, Intro, Profile, Directory, Economic ProposalMelody Kaye MonsantoPas encore d'évaluation
- G CP CompiledDocument120 pagesG CP CompiledMelody Kaye MonsantoPas encore d'évaluation
- Chapter 1 ECG For StudentsDocument47 pagesChapter 1 ECG For StudentsMelody Kaye MonsantoPas encore d'évaluation
- "Change" (A Synthesis Paper) in Partial Fulfillment of The Requirements in FFPDocument4 pages"Change" (A Synthesis Paper) in Partial Fulfillment of The Requirements in FFPMelody Kaye MonsantoPas encore d'évaluation
- Acute Pain..Document2 pagesAcute Pain..Melody Kaye MonsantoPas encore d'évaluation
- Pa Tho PhysiologyDocument3 pagesPa Tho PhysiologyMelody Kaye MonsantoPas encore d'évaluation
- Acute Pain..Document2 pagesAcute Pain..Melody Kaye MonsantoPas encore d'évaluation
- Allergic DisordersDocument3 pagesAllergic DisordersMelody Kaye MonsantoPas encore d'évaluation
- Invitation OutlineDocument1 pageInvitation OutlineMelody Kaye MonsantoPas encore d'évaluation
- A Moment Like This LyricsDocument2 pagesA Moment Like This LyricsMelody Kaye MonsantoPas encore d'évaluation
- PathophysiologyDocument1 pagePathophysiologyMelody Kaye MonsantoPas encore d'évaluation
- The Philippine NUrsing Act of 2002 Aka R.A. 9173Document7 pagesThe Philippine NUrsing Act of 2002 Aka R.A. 9173Rho Vince Caño MalagueñoPas encore d'évaluation
- Infectious Diseases GuideDocument30 pagesInfectious Diseases GuideSarahPas encore d'évaluation
- HydronephrosisDocument15 pagesHydronephrosisAdetz HaedetzPas encore d'évaluation
- Concepts in Dental Public Health CH 1Document23 pagesConcepts in Dental Public Health CH 1Maria Mercedes LeivaPas encore d'évaluation
- مدونة كل العرب الطبية Davidson - Mcq - 22 - edition PDFDocument232 pagesمدونة كل العرب الطبية Davidson - Mcq - 22 - edition PDFنورهانعزالدين100% (1)
- Alt Ast Alp GGT Pada Liver DiseaseDocument5 pagesAlt Ast Alp GGT Pada Liver DiseaseNararto PrijogoPas encore d'évaluation
- Wang Et Al. - 2020 - Time Series Prediction For The Epidemic Trends of COVID-19 Using The Improved LSTM Deep Learning Method Case Stu (2) - AnnotatedDocument8 pagesWang Et Al. - 2020 - Time Series Prediction For The Epidemic Trends of COVID-19 Using The Improved LSTM Deep Learning Method Case Stu (2) - AnnotatedZipeng WuPas encore d'évaluation
- Application Form Health Examination Form Parents Consent FormDocument1 pageApplication Form Health Examination Form Parents Consent Formapril rose catainaPas encore d'évaluation
- Managing Acute Meningitis: HistoryDocument37 pagesManaging Acute Meningitis: HistoryMhelshy VillanuevaPas encore d'évaluation
- Event 201 Johns Hopkins Center For Health SecurityDocument1 pageEvent 201 Johns Hopkins Center For Health SecurityDan CPas encore d'évaluation
- Cardiovascular SystemDocument100 pagesCardiovascular SystemTerence ValdehuezaPas encore d'évaluation
- Progressive Balbar Palsy: Dr. Mohamed Ali 3 Year MD IM ResidentDocument15 pagesProgressive Balbar Palsy: Dr. Mohamed Ali 3 Year MD IM ResidentMohamed AliPas encore d'évaluation
- SADES18 DikonversiDocument90 pagesSADES18 DikonversiIc-tika Siee ChuabbiePas encore d'évaluation
- Evaluation of A Patient With Vitreous HaemorrhageDocument5 pagesEvaluation of A Patient With Vitreous HaemorrhageLisa MayasariPas encore d'évaluation
- Septicemia NewDocument3 pagesSepticemia NewkainatPas encore d'évaluation
- How the Black Death Changed Medieval EuropeDocument5 pagesHow the Black Death Changed Medieval EuropeRandi JeanPas encore d'évaluation
- Infection Control in Dental Practice 2009Document3 pagesInfection Control in Dental Practice 2009wildernest1Pas encore d'évaluation
- Chapter 14: Principles of Disease and EpidemiologyDocument53 pagesChapter 14: Principles of Disease and EpidemiologyAbhishek Isaac MathewPas encore d'évaluation
- ScabiesDocument1 pageScabiesMarco Antonio KoffPas encore d'évaluation
- Phrasal Verbs 1Document4 pagesPhrasal Verbs 1Steven DaviesPas encore d'évaluation
- Plastida Mitokondria 11 PDFDocument29 pagesPlastida Mitokondria 11 PDFelsaPas encore d'évaluation
- Case River BlindnessDocument2 pagesCase River BlindnessMuhd ZawirPas encore d'évaluation
- Capacity RestrictionsDocument1 pageCapacity Restrictions9newsPas encore d'évaluation