Vous aimerez peut-être aussi
- Rheumatic Endocarditis: o o o o oDocument5 pagesRheumatic Endocarditis: o o o o ogaratoh099Pas encore d'évaluation
- Acute Rheumatic FeverDocument9 pagesAcute Rheumatic FeverHarish Kumar KumawatPas encore d'évaluation
- Pneumothorax, Tension and TraumaticDocument24 pagesPneumothorax, Tension and TraumaticSatria WibawaPas encore d'évaluation
- Disseminated Intravascular Coagulation (DIC)Document24 pagesDisseminated Intravascular Coagulation (DIC)Atiya HajjajPas encore d'évaluation
- Venous Thromboembolism (VTE) - McMaster Pathophysiology ReviewDocument9 pagesVenous Thromboembolism (VTE) - McMaster Pathophysiology ReviewFadiyah UlfahPas encore d'évaluation
- Systemic Lupus ErythematosusDocument46 pagesSystemic Lupus ErythematosuspriscillaPas encore d'évaluation
- CA Emergency: Tumor Lysis SyndromeDocument9 pagesCA Emergency: Tumor Lysis SyndromeJai - HoPas encore d'évaluation
- Diagnostic TestsDocument6 pagesDiagnostic TestsKelsey MacaraigPas encore d'évaluation
- Normal Values of CBCDocument1 pageNormal Values of CBCCherr NollPas encore d'évaluation
- CKD Guide: Risks, Stages, and Management of Chronic Kidney DiseaseDocument54 pagesCKD Guide: Risks, Stages, and Management of Chronic Kidney DiseaseJosh Matthew RosalesPas encore d'évaluation
- Nutrition Through The Life SpanDocument5 pagesNutrition Through The Life SpanBcore BikoPas encore d'évaluation
- Pathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsDocument2 pagesPathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsAb Staholic Boii100% (1)
- Schematic Diagram of The Pathophysiology of Toxic Shock SyndromeDocument2 pagesSchematic Diagram of The Pathophysiology of Toxic Shock SyndromeRan MaPas encore d'évaluation
- Pathogenesis of Severe Dengue InfectionDocument4 pagesPathogenesis of Severe Dengue InfectionAhmed MawardiPas encore d'évaluation
- 01 EnemaDocument4 pages01 Enemabunso padillaPas encore d'évaluation
- LeptospirosisDocument13 pagesLeptospirosis천사천사Pas encore d'évaluation
- Disseminated Intravascular CoagulationDocument2 pagesDisseminated Intravascular CoagulationVince100% (1)
- DB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaDocument5 pagesDB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaNeil Alcazaren かわいいPas encore d'évaluation
- E HealthDocument7 pagesE HealthLorilla AlvinPas encore d'évaluation
- Idiopathic Thrombocytopenic Purpura: Overview With Report of A CaseDocument4 pagesIdiopathic Thrombocytopenic Purpura: Overview With Report of A CaseHernan GonzalezPas encore d'évaluation
- Hepatic EncephalopathyDocument3 pagesHepatic EncephalopathyAnonymous GIGXKjfLPas encore d'évaluation
- Stevens Johnson DiseaseDocument5 pagesStevens Johnson DiseaseShammy RNPas encore d'évaluation
- Hanta Vi Ru S Inf Ection SDocument20 pagesHanta Vi Ru S Inf Ection Stummalapalli venkateswara rao100% (3)
- GlomerulonephritisDocument4 pagesGlomerulonephritisMary Cris BasayaPas encore d'évaluation
- 3M CVP Monitoring - Assisting in BMA ECG Interpretation - Final Draft - 3CDocument65 pages3M CVP Monitoring - Assisting in BMA ECG Interpretation - Final Draft - 3CAlexa GoteraPas encore d'évaluation
- Idiopathic Thrombocytopenic Purpura (ITP)Document7 pagesIdiopathic Thrombocytopenic Purpura (ITP)Rizqka PertiwiPas encore d'évaluation
- Acute Post Streptococcal Glomerulonephritis APSGNDocument16 pagesAcute Post Streptococcal Glomerulonephritis APSGNErlin IrawatiPas encore d'évaluation
- RabiesDocument10 pagesRabiesWinda LiraPas encore d'évaluation
- Essensial Hypertension Pathogenesis and PathophsiologyDocument22 pagesEssensial Hypertension Pathogenesis and PathophsiologyAmeliana KamaludinPas encore d'évaluation
- Rheumatic FeverDocument56 pagesRheumatic Feveralmawang100% (1)
- Reviewer Chap 49 Fecal EliminationDocument3 pagesReviewer Chap 49 Fecal EliminationKeren GaciasPas encore d'évaluation
- Liver CirrhosisDocument30 pagesLiver CirrhosisMelody PardilloPas encore d'évaluation
- Infective Endocarditis CaseDocument3 pagesInfective Endocarditis CaseMershen GaniaPas encore d'évaluation
- DIC Case StudyDocument7 pagesDIC Case StudyRobertPas encore d'évaluation
- Water-Soluble VitaminsDocument4 pagesWater-Soluble VitaminsVasile IonPas encore d'évaluation
- Cor PulmonaleDocument21 pagesCor Pulmonalemaibejose100% (1)
- Microbiology Lab #1 - StainingDocument85 pagesMicrobiology Lab #1 - StainingAmanda PachecoPas encore d'évaluation
- Cardiorenal SyndromeDocument89 pagesCardiorenal SyndromeGabriyah HamzahPas encore d'évaluation
- DAY 2 Febrile Seizure Kuliah MHSDocument45 pagesDAY 2 Febrile Seizure Kuliah MHSAdhi WiratmaPas encore d'évaluation
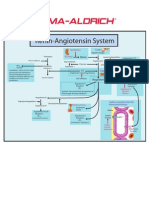
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Dr. Sunatrio - Management Hypovolemic ShockDocument59 pagesDr. Sunatrio - Management Hypovolemic ShockArga Putra SaboePas encore d'évaluation
- ICU Rounds: Pulmonary Leukostasis as a Complication of LeukemiaDocument6 pagesICU Rounds: Pulmonary Leukostasis as a Complication of LeukemiaPratita Jati PermatasariPas encore d'évaluation
- Ventikular Septal Defect FixDocument18 pagesVentikular Septal Defect FixPutri Sari DewiPas encore d'évaluation
- Cardiorenal SyndromeDocument8 pagesCardiorenal SyndromeJeremia KurniawanPas encore d'évaluation
- Fluid RequiermentDocument14 pagesFluid RequiermentKrini TandelPas encore d'évaluation
- Case Study Anemia-1Document6 pagesCase Study Anemia-1Melsya H UtamiPas encore d'évaluation
- Case 2Document4 pagesCase 2Kim Ruiz100% (1)
- Kuliah Thrombosis 2015 NNDocument39 pagesKuliah Thrombosis 2015 NNBeladiena Citra SiregarPas encore d'évaluation
- AMLDocument19 pagesAMLquerokeropi100% (1)
- Cardiomyopathy 1223958636063843 9Document87 pagesCardiomyopathy 1223958636063843 9Dainy ThomasPas encore d'évaluation
- Mechanism of HypertensionDocument4 pagesMechanism of HypertensionAlya Putri KhairaniPas encore d'évaluation
- Causes and Pathophysiology of Congestive Heart Failure (CHFDocument1 pageCauses and Pathophysiology of Congestive Heart Failure (CHFLance MarquezPas encore d'évaluation
- Bartter Syndrome: Rare Inherited Kidney DisorderDocument3 pagesBartter Syndrome: Rare Inherited Kidney DisorderEnny Andriani100% (1)
- LECTURES Liver PathophysiologyDocument118 pagesLECTURES Liver PathophysiologyTarik100% (1)
- Acute and Chronic Pancreatitis ShirleyDocument6 pagesAcute and Chronic Pancreatitis ShirleyVictor AladejanaPas encore d'évaluation
- By DR - Tosif Ahmad TMO-PediatricsDocument27 pagesBy DR - Tosif Ahmad TMO-PediatricskamalPas encore d'évaluation
- Nephrotic Syndrome 2016Document45 pagesNephrotic Syndrome 2016alaaPas encore d'évaluation
- Rheumatic Fever Is AnDocument7 pagesRheumatic Fever Is AnHamza SaeedPas encore d'évaluation
- Rheumatic FeverDocument6 pagesRheumatic FeverSam AraPas encore d'évaluation
- Rheumatic Fever (Caypuno, Isaac-Lee P.)Document15 pagesRheumatic Fever (Caypuno, Isaac-Lee P.)Carlojay IniegoPas encore d'évaluation
- What Is The Purpose of A Sternum RubDocument1 pageWhat Is The Purpose of A Sternum RubKelvin KurtPas encore d'évaluation
- Female Reproductive Cycle StagesDocument2 pagesFemale Reproductive Cycle StagesKelvin KurtPas encore d'évaluation
- Postpartum Care GuideDocument10 pagesPostpartum Care GuideKelvin KurtPas encore d'évaluation
- IV. Intrapartal CareDocument7 pagesIV. Intrapartal CareKelvin KurtPas encore d'évaluation
- BacteriaDocument4 pagesBacteriaKelvin KurtPas encore d'évaluation
- ANTI OBESITY CAMPDocument13 pagesANTI OBESITY CAMPgirishlambaPas encore d'évaluation
- Mohamed Ali El Maroush PH.D of Prosthodontic & Maxillofacial (Ain Shams University)Document38 pagesMohamed Ali El Maroush PH.D of Prosthodontic & Maxillofacial (Ain Shams University)Ňøoř ĄłhųdàPas encore d'évaluation
- African Lion (Panthera Leo) With Dark Mane. Photo Credit: Dr. Michelle StevensDocument45 pagesAfrican Lion (Panthera Leo) With Dark Mane. Photo Credit: Dr. Michelle StevensWaqar IbrahimPas encore d'évaluation
- Anaesthesia For Paediatric Dentistry: Lola Adewale MBCHB DCH FrcaDocument8 pagesAnaesthesia For Paediatric Dentistry: Lola Adewale MBCHB DCH FrcaJavier Farias VeraPas encore d'évaluation
- SchistosomaDocument5 pagesSchistosomasarguss14100% (1)
- 2009 Nec Hiv Dec Aidsreg2009Document3 pages2009 Nec Hiv Dec Aidsreg2009Jing CruzPas encore d'évaluation
- 4 InterviewDocument8 pages4 Interviewapi-359161098Pas encore d'évaluation
- Zebra PDFDocument10 pagesZebra PDFelmond mortaPas encore d'évaluation
- The Homeopathic Treatment of LymeDocument31 pagesThe Homeopathic Treatment of LymeMartoufi100% (2)
- Circulation in Humans ExplainedDocument2 pagesCirculation in Humans ExplainedKliemmah PeltierPas encore d'évaluation
- Statement From Maine Veterinary Medical CenterDocument3 pagesStatement From Maine Veterinary Medical CenterWGMEPas encore d'évaluation
- Early Human DietsDocument3 pagesEarly Human DietsDouglas CamposPas encore d'évaluation
- Aasha Ram BapuDocument10 pagesAasha Ram BapussmaddiPas encore d'évaluation
- Diagnostic MethodsDocument93 pagesDiagnostic MethodsSyukri La Ranti100% (3)
- Bab 5 - AkuakulturTDocument63 pagesBab 5 - AkuakulturTNor FaizahPas encore d'évaluation
- 1166 Stomach Dr.-RaviDocument38 pages1166 Stomach Dr.-RaviKubra ĖdrisPas encore d'évaluation
- Alexander Holschneider, Prem Puri - Hirschprung Disease and Allied DisordersDocument510 pagesAlexander Holschneider, Prem Puri - Hirschprung Disease and Allied DisordersDiana Lora ParvuPas encore d'évaluation
- Goat Farming 2004Document154 pagesGoat Farming 2004Jahn Symon RiveraPas encore d'évaluation
- Polio OutbreakDocument3 pagesPolio OutbreakAyn Jel MayPas encore d'évaluation
- Darwins Voyage PowerPoint For WebsiteDocument38 pagesDarwins Voyage PowerPoint For WebsiteEko SujatmikoPas encore d'évaluation
- These Nouns Are The Names For A Collection of Things. Which Are True?Document11 pagesThese Nouns Are The Names For A Collection of Things. Which Are True?Muhammad Ariff Aizuddin AbdullahPas encore d'évaluation
- LIVERDocument18 pagesLIVERShivaniLeela100% (3)
- Hpai FlyerDocument2 pagesHpai FlyerTed BakerPas encore d'évaluation
- Viral Diseases and the Immune SystemDocument27 pagesViral Diseases and the Immune SystemHendika Ariyo SPas encore d'évaluation
- Organ Systems 1 NBC ReviewerDocument39 pagesOrgan Systems 1 NBC ReviewerJames ChavezPas encore d'évaluation
- List Procedur ICD-9CMDocument336 pagesList Procedur ICD-9CMabdiPas encore d'évaluation
- OBDocument4 pagesOBCharlie Cotoner FalgueraPas encore d'évaluation
- February 17, 2017 Strathmore TimesDocument24 pagesFebruary 17, 2017 Strathmore TimesStrathmore TimesPas encore d'évaluation
- CRI Annual Report 2006Document10 pagesCRI Annual Report 2006aptureincPas encore d'évaluation
- Alveolar Osteitis A Comprehensive Review ofDocument10 pagesAlveolar Osteitis A Comprehensive Review ofFakhrul ImamPas encore d'évaluation
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionD'EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionÉvaluation : 4 sur 5 étoiles4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (13)
- The Comfort of Crows: A Backyard YearD'EverandThe Comfort of Crows: A Backyard YearÉvaluation : 4.5 sur 5 étoiles4.5/5 (23)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsD'EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsÉvaluation : 3.5 sur 5 étoiles3.5/5 (3)
- Why We Die: The New Science of Aging and the Quest for ImmortalityD'EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (78)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeD'EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BePas encore d'évaluation
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsD'EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Techniques Exercises And Tricks For Memory ImprovementD'EverandTechniques Exercises And Tricks For Memory ImprovementÉvaluation : 4.5 sur 5 étoiles4.5/5 (40)
- The Obesity Code: Unlocking the Secrets of Weight LossD'EverandThe Obesity Code: Unlocking the Secrets of Weight LossÉvaluation : 5 sur 5 étoiles5/5 (4)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisD'EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (1)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisD'EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisÉvaluation : 5 sur 5 étoiles5/5 (8)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsD'EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsÉvaluation : 4.5 sur 5 étoiles4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingD'EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (33)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsD'EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsPas encore d'évaluation
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingD'EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingÉvaluation : 5 sur 5 étoiles5/5 (5)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.D'EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Évaluation : 4.5 sur 5 étoiles4.5/5 (110)
- The Ultimate Guide To Memory Improvement TechniquesD'EverandThe Ultimate Guide To Memory Improvement TechniquesÉvaluation : 5 sur 5 étoiles5/5 (34)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaD'EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeD'EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeÉvaluation : 4.5 sur 5 étoiles4.5/5 (253)
- The Happiness Trap: How to Stop Struggling and Start LivingD'EverandThe Happiness Trap: How to Stop Struggling and Start LivingÉvaluation : 4 sur 5 étoiles4/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsD'EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsPas encore d'évaluation
- Recovering from Emotionally Immature Parents: Practical Tools to Establish Boundaries and Reclaim Your Emotional AutonomyD'EverandRecovering from Emotionally Immature Parents: Practical Tools to Establish Boundaries and Reclaim Your Emotional AutonomyÉvaluation : 4.5 sur 5 étoiles4.5/5 (201)
- The Tennis Partner: A Doctor's Story of Friendship and LossD'EverandThe Tennis Partner: A Doctor's Story of Friendship and LossÉvaluation : 4.5 sur 5 étoiles4.5/5 (4)