Vous aimerez peut-être aussi
- Medicare Part B Premium Fact SheetDocument2 pagesMedicare Part B Premium Fact SheetTerry PetersonPas encore d'évaluation
- 2010-04-02 - Health Care Reform ArticleDocument4 pages2010-04-02 - Health Care Reform ArticleTerry PetersonPas encore d'évaluation
- ND SSI StatsDocument2 pagesND SSI StatsTerry PetersonPas encore d'évaluation
- IRWE Request TemplateDocument3 pagesIRWE Request TemplateTerry PetersonPas encore d'évaluation
- Bylaws of SCGC - 2010Document17 pagesBylaws of SCGC - 2010Terry PetersonPas encore d'évaluation
- Fy09 DFC Final RfaDocument99 pagesFy09 DFC Final RfaTerry Peterson100% (1)
- Blind Work Expense RequestDocument2 pagesBlind Work Expense RequestTerry PetersonPas encore d'évaluation
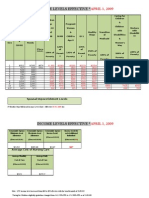
- IM 5062 ATTACHED CHART 2009 Medicaid Income Level Chart - Effective 04-01-09Document2 pagesIM 5062 ATTACHED CHART 2009 Medicaid Income Level Chart - Effective 04-01-09Terry Peterson100% (1)
- Earnings Release 82508 (1) - MarkDocument1 pageEarnings Release 82508 (1) - MarkTerry PetersonPas encore d'évaluation
- BPQY Release 90508 Final IIDocument2 pagesBPQY Release 90508 Final IITerry PetersonPas encore d'évaluation
- Deeming Chart 2009Document1 pageDeeming Chart 2009Terry Peterson100% (3)
- Earnings Release 82508 (1) - MarkDocument1 pageEarnings Release 82508 (1) - MarkTerry PetersonPas encore d'évaluation
- BPQY Release 90808 #1Document1 pageBPQY Release 90808 #1Terry PetersonPas encore d'évaluation
- Earnings Release 82508 #2Document1 pageEarnings Release 82508 #2Terry PetersonPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Eligibility Results NoticeDocument12 pagesEligibility Results NoticeLagannPas encore d'évaluation
- Annexure 1Document4 pagesAnnexure 1Mahmud Abdullahi SarkiPas encore d'évaluation
- Harvard Case Study-YashaswiniDocument5 pagesHarvard Case Study-Yashaswiniankit__bansal100% (1)
- Philippine Health Insurance CorporationDocument7 pagesPhilippine Health Insurance CorporationEllen Glae DaquipilPas encore d'évaluation
- PORTO Esn Survival GuideDocument84 pagesPORTO Esn Survival GuideLuciana MonteiroPas encore d'évaluation
- 80D CertificateDocument2 pages80D CertificateYogy YPas encore d'évaluation
- Web Aggregator SyllabusDocument5 pagesWeb Aggregator Syllabussam franklinPas encore d'évaluation
- 2017 HHS Poverty Guidelines For Affidavit of SupportDocument1 page2017 HHS Poverty Guidelines For Affidavit of SupportLiz MPas encore d'évaluation
- Medical Insurance TerminologyDocument4 pagesMedical Insurance TerminologyGene'sPas encore d'évaluation
- A Critical Insight, Analysis and Comparative of Health Care Provision in The United Kingdom and United States of America.Document19 pagesA Critical Insight, Analysis and Comparative of Health Care Provision in The United Kingdom and United States of America.Abiola AbrahamPas encore d'évaluation
- HCF Mid ExtrasDocument3 pagesHCF Mid Extrasnoneother2Pas encore d'évaluation
- Claim Form For Health Insurance Policies - Part A Name of Insurance Company: Client NameDocument4 pagesClaim Form For Health Insurance Policies - Part A Name of Insurance Company: Client NameSatyadev KalraPas encore d'évaluation
- Orange Grey Medical PresentationDocument10 pagesOrange Grey Medical PresentationRajPas encore d'évaluation
- Sample Part A Medicare Summary NoticeDocument6 pagesSample Part A Medicare Summary NoticejerilPas encore d'évaluation
- INSURANCE EXAM REVIEWDocument6 pagesINSURANCE EXAM REVIEWJon EsberPas encore d'évaluation
- Understanding The ACA's Health Care ExchangesDocument10 pagesUnderstanding The ACA's Health Care ExchangesMarketingRCAPas encore d'évaluation
- Viva HimejiDocument19 pagesViva Himejiapi-451489221Pas encore d'évaluation
- BCBSTX Ineligible Reason Code ListDocument34 pagesBCBSTX Ineligible Reason Code ListmrehmanPas encore d'évaluation
- Health Law OutlineDocument28 pagesHealth Law OutlineJenna Burch83% (6)
- Kentucky: Medicare Advantage Cost Plans and DemonstrationsDocument46 pagesKentucky: Medicare Advantage Cost Plans and Demonstrationsanon-76504Pas encore d'évaluation
- Revenue CycleDocument0 pageRevenue Cyclecasti134Pas encore d'évaluation
- IHOMP Self Assessment ToolDocument7 pagesIHOMP Self Assessment ToolPhilip Duremdes Doromal80% (5)
- 6.3. Burden of Out-Of-Pocket Health Expenditure: 6. Access To CareDocument3 pages6.3. Burden of Out-Of-Pocket Health Expenditure: 6. Access To CareNawaz RasoolPas encore d'évaluation
- Cambay Spa & Resort, UdaipurDocument2 pagesCambay Spa & Resort, UdaipurCambay Hotels & ResortsPas encore d'évaluation
- Insurance - Fire PolicyDocument4 pagesInsurance - Fire PolicyPrasad GharatPas encore d'évaluation
- 80-194 Medicaid Eligibility Examiner 2daDocument3 pages80-194 Medicaid Eligibility Examiner 2daMehmood J SheikhPas encore d'évaluation
- PCE - Part B General InsuranceDocument125 pagesPCE - Part B General InsuranceAshlee JingPas encore d'évaluation
- Ub-04 Chars ManualDocument82 pagesUb-04 Chars ManualVeeresh BikkanetiPas encore d'évaluation
- Types of Insurance PowerPoint 1.10.1.G1Document32 pagesTypes of Insurance PowerPoint 1.10.1.G1Bilal Uddin ShinwariPas encore d'évaluation
- For In-Home Supportive Services Workers: PASC-SEIU Homecare Workers Health Care PlanDocument9 pagesFor In-Home Supportive Services Workers: PASC-SEIU Homecare Workers Health Care PlanMustaffah KabelyyonPas encore d'évaluation