Vous aimerez peut-être aussi
- Colado, Athlete CoreDocument9 pagesColado, Athlete CorePhooi Yee LauPas encore d'évaluation
- Hu, ASLR Healthy PDFDocument7 pagesHu, ASLR Healthy PDFPhooi Yee LauPas encore d'évaluation
- RMQ English (Original)Document2 pagesRMQ English (Original)Phooi Yee LauPas encore d'évaluation
- Pre Operative Pelvis ExerciseDocument1 pagePre Operative Pelvis ExercisePhooi Yee LauPas encore d'évaluation
- 5 StsDocument13 pages5 StsPhooi Yee LauPas encore d'évaluation
- Lumbar MultifidusDocument6 pagesLumbar Multifidussridhar100% (1)
- Oconnelletal2017, Backpain GuildelineDocument14 pagesOconnelletal2017, Backpain GuildelinePhooi Yee LauPas encore d'évaluation
- Plantartaping PDFDocument2 pagesPlantartaping PDFPhooi Yee LauPas encore d'évaluation
- Multom Rat Running PDFDocument8 pagesMultom Rat Running PDFPhooi Yee LauPas encore d'évaluation
- Paillard PostureDocument3 pagesPaillard PosturePhooi Yee LauPas encore d'évaluation
- DiGiovanni 2003 PDFDocument8 pagesDiGiovanni 2003 PDFPhooi Yee LauPas encore d'évaluation
- Training To Optimize Performance Driving Reorganization?: Exercise and Functional in Stroke: NeuralDocument10 pagesTraining To Optimize Performance Driving Reorganization?: Exercise and Functional in Stroke: NeuralPhooi Yee LauPas encore d'évaluation
- Neuro ExerciseDocument7 pagesNeuro ExercisePhooi Yee LauPas encore d'évaluation
- Urquhart, TR A PDFDocument9 pagesUrquhart, TR A PDFPhooi Yee LauPas encore d'évaluation
- Bourcher, NeckpainbalanceDocument7 pagesBourcher, NeckpainbalancePhooi Yee LauPas encore d'évaluation
- DBE Movement PDFDocument12 pagesDBE Movement PDFPhooi Yee LauPas encore d'évaluation
- Frost, Low Back Pain BalanceDocument7 pagesFrost, Low Back Pain BalancePhooi Yee LauPas encore d'évaluation
- Pinsault, Neck MuscleDocument9 pagesPinsault, Neck MusclePhooi Yee LauPas encore d'évaluation
- Vuillerme, Cervical PostureDocument5 pagesVuillerme, Cervical PosturePhooi Yee LauPas encore d'évaluation
- Stress QuestionnaireDocument2 pagesStress QuestionnaireCalin Popa100% (1)
- Dehner, NeckbalanceDocument7 pagesDehner, NeckbalancePhooi Yee LauPas encore d'évaluation
- Merger, Eye MVTDocument11 pagesMerger, Eye MVTPhooi Yee LauPas encore d'évaluation
- Kogler, NeckbalanceDocument6 pagesKogler, NeckbalancePhooi Yee LauPas encore d'évaluation
- Hellstrom, Neck SymphtaticDocument15 pagesHellstrom, Neck SymphtaticPhooi Yee LauPas encore d'évaluation
- Kristenen, NeckmusclebalanceDocument9 pagesKristenen, NeckmusclebalancePhooi Yee LauPas encore d'évaluation
- Hellstrom, Neck SymphtaticDocument15 pagesHellstrom, Neck SymphtaticPhooi Yee LauPas encore d'évaluation
- Schimid - Neck Muscle PostureDocument13 pagesSchimid - Neck Muscle PosturePhooi Yee LauPas encore d'évaluation
- Humphreys, Cervicaloutcome For BalanceDocument7 pagesHumphreys, Cervicaloutcome For BalancePhooi Yee LauPas encore d'évaluation
- Kogler, NeckbalanceDocument6 pagesKogler, NeckbalancePhooi Yee LauPas encore d'évaluation
- Yamagata, Neck ReflexDocument4 pagesYamagata, Neck ReflexPhooi Yee LauPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Solid Modeling Techniques: Constructive Solid Geometry (CSG)Document22 pagesSolid Modeling Techniques: Constructive Solid Geometry (CSG)amolPas encore d'évaluation
- Digital Signal Processing: B.E Ece (5Th Semester)Document17 pagesDigital Signal Processing: B.E Ece (5Th Semester)Saatwat CoolPas encore d'évaluation
- BECO UACE Chem2Document6 pagesBECO UACE Chem2EMMANUEL BIRUNGIPas encore d'évaluation
- Eliminating Oscillation Between Parallel MnosfetsDocument6 pagesEliminating Oscillation Between Parallel MnosfetsCiprian BirisPas encore d'évaluation
- Sw34 Religion, Secularism and The Environment by NasrDocument19 pagesSw34 Religion, Secularism and The Environment by Nasrbawah61455Pas encore d'évaluation
- Mini-Case 1 Ppe AnswerDocument11 pagesMini-Case 1 Ppe Answeryu choong100% (2)
- Germania Agenturinfo enDocument4 pagesGermania Agenturinfo enДушан СтепановићPas encore d'évaluation
- ChipmunkDocument19 pagesChipmunkema.nemec13Pas encore d'évaluation
- 10th ORLIAC Scientific Program As of 26 Jan 2018Document6 pages10th ORLIAC Scientific Program As of 26 Jan 2018AyuAnatrieraPas encore d'évaluation
- Ii 2015 1Document266 pagesIi 2015 1tuni santePas encore d'évaluation
- Frontinus - Water Management of RomeDocument68 pagesFrontinus - Water Management of RomezElfmanPas encore d'évaluation
- MiscanthusDocument27 pagesMiscanthusJacob GuerraPas encore d'évaluation
- Trawl Master Present A TieDocument19 pagesTrawl Master Present A Tieapi-3719203Pas encore d'évaluation
- Bhagwati School Strap Report AnalysisDocument60 pagesBhagwati School Strap Report AnalysisReverse Minded100% (1)
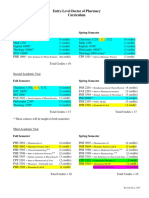
- Pharmd CurriculumDocument18 pagesPharmd Curriculum5377773Pas encore d'évaluation
- Tuesday, 16 November 2021 - Afternoon Discovering ElectronicsDocument20 pagesTuesday, 16 November 2021 - Afternoon Discovering Electronicsnvmalt070Pas encore d'évaluation
- LJ-V7080 DatasheetDocument2 pagesLJ-V7080 DatasheetOrhan DenizliPas encore d'évaluation
- Upaam 1135891 202105060749199700Document18 pagesUpaam 1135891 202105060749199700Kartik KapoorPas encore d'évaluation
- Understanding Bernoulli's Principle Through Simulations PDFDocument4 pagesUnderstanding Bernoulli's Principle Through Simulations PDFIoannis GaroufalidisPas encore d'évaluation
- Aircraft Design Course PhillStocking 4.2Document48 pagesAircraft Design Course PhillStocking 4.2ugurugur1982Pas encore d'évaluation
- Serial Analysis of Gene Expression (SAGE)Document34 pagesSerial Analysis of Gene Expression (SAGE)Rohit PhalakPas encore d'évaluation
- Binet Kamat Test For General Mental AbilitiesDocument54 pagesBinet Kamat Test For General Mental AbilitiesSana Siddiq100% (14)
- Mathematical Modeling of Mechanical Systems and Electrical SystemsDocument49 pagesMathematical Modeling of Mechanical Systems and Electrical SystemsMary DunhamPas encore d'évaluation
- Communication Guide: For Vita 62 Compliant VPX Power SuppliesDocument8 pagesCommunication Guide: For Vita 62 Compliant VPX Power Suppliesk.saikumarPas encore d'évaluation
- THE WEATHER LISTENING - Stalin GuañunaDocument1 pageTHE WEATHER LISTENING - Stalin GuañunaSTALIN JESUS GUA�UNA CHICAIZAPas encore d'évaluation
- Relationsh Between EM and Young S ModuliDocument7 pagesRelationsh Between EM and Young S ModuliDwight AndersonPas encore d'évaluation
- Propert 447-445Document11 pagesPropert 447-445LUNA100% (1)
- Chapter Three: 1 - The Coarse Grain SoilsDocument21 pagesChapter Three: 1 - The Coarse Grain SoilsSalih MohayaddinPas encore d'évaluation
- RUKUS April 2011Document40 pagesRUKUS April 2011RUKUS Magazine100% (2)
- The Wild T1 TheodoliteDocument61 pagesThe Wild T1 TheodoliteCJLara100% (1)