Vous aimerez peut-être aussi
- Cyber-Physical Attacks: A Growing Invisible ThreatD'EverandCyber-Physical Attacks: A Growing Invisible ThreatÉvaluation : 4.5 sur 5 étoiles4.5/5 (3)
- Incident InvestDocument8 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Incident InvestDocument16 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Incident InvestDocument15 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Appendix G: Quick Checklist For InvestigatorsDocument5 pagesAppendix G: Quick Checklist For InvestigatorsAndy DolmanPas encore d'évaluation
- Incident InvestDocument17 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Incident InvestDocument16 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Continuous Improvement For The Incident Investigation SystemDocument10 pagesContinuous Improvement For The Incident Investigation SystemAndy DolmanPas encore d'évaluation
- All Accident Are IncidentDocument6 pagesAll Accident Are IncidenttemterPas encore d'évaluation
- Fault Tree AnalysisDocument7 pagesFault Tree AnalysisthawdarPas encore d'évaluation
- Root Cause Analysis: Ruksana Hamid, Medical Officer and Anesthesiologist, JK HealthDocument7 pagesRoot Cause Analysis: Ruksana Hamid, Medical Officer and Anesthesiologist, JK HealthAnar HajiyevPas encore d'évaluation
- Lec 47Document40 pagesLec 47Arul PrasaadPas encore d'évaluation
- Accident Causation Theories and ConceptDocument4 pagesAccident Causation Theories and ConceptShayne Aira AnggongPas encore d'évaluation
- Risk-Based Approach To Near Miss: Safety ManagementDocument0 pageRisk-Based Approach To Near Miss: Safety ManagementLovePas encore d'évaluation
- SHM - Practical 12 - Risk Assessment MethodsDocument8 pagesSHM - Practical 12 - Risk Assessment MethodsBhaliya AadityaPas encore d'évaluation
- Accident Analysis TechniquesDocument22 pagesAccident Analysis Techniquesbyron eugenioPas encore d'évaluation
- Quality of Incident InvestigationsDocument4 pagesQuality of Incident InvestigationsJose Martin ChaconPas encore d'évaluation
- Theory of Accident CausesDocument3 pagesTheory of Accident CausesvuongPas encore d'évaluation
- FTA in Probability Safety ManagementDocument3 pagesFTA in Probability Safety Managementlydiaqwerty1234Pas encore d'évaluation
- HSE Human Factors Briefing Note No. 3 Humans and RiskDocument6 pagesHSE Human Factors Briefing Note No. 3 Humans and RiskSayed DarwishPas encore d'évaluation
- Michael Tooma Incident Investigation2012Document66 pagesMichael Tooma Incident Investigation2012Saloka ArioPas encore d'évaluation
- Chapter 5 (Accident Causation and Investigation)Document22 pagesChapter 5 (Accident Causation and Investigation)Anonymous 8NSojGPas encore d'évaluation
- HSE Human Factors Briefing Note No. 3 Humans and RiskDocument6 pagesHSE Human Factors Briefing Note No. 3 Humans and Riskjoaonunes.405443Pas encore d'évaluation
- Golden Rules of Process SafetyDocument1 pageGolden Rules of Process SafetyLau ZamPas encore d'évaluation
- Root Cause AnalysisDocument19 pagesRoot Cause AnalysisMentari Putri PertiwiPas encore d'évaluation
- Causal Analysis On Herald of Free Enterprise'S Disaster: A Stamp-Based ApproachDocument11 pagesCausal Analysis On Herald of Free Enterprise'S Disaster: A Stamp-Based ApproachSU SHIPONPas encore d'évaluation
- Systems Thinking in Risk ManagementDocument11 pagesSystems Thinking in Risk Managementalberto_cohenPas encore d'évaluation
- BSCATpaperassubmitteddec 82014Document15 pagesBSCATpaperassubmitteddec 82014Moroko69Pas encore d'évaluation
- Accident Causation TheoryDocument4 pagesAccident Causation TheoryzombiePas encore d'évaluation
- Root Cause AnalysisDocument7 pagesRoot Cause Analysisolivia523Pas encore d'évaluation
- Rauof 1998 - Theory of Accident Causes PDFDocument4 pagesRauof 1998 - Theory of Accident Causes PDFGustavo DucaPas encore d'évaluation
- 4.2b - Risk AssessmentDocument11 pages4.2b - Risk Assessmentkenoly123Pas encore d'évaluation
- On A Difficulty of Intrusion DetectionDocument10 pagesOn A Difficulty of Intrusion DetectionRick WhitePas encore d'évaluation
- Safety Management System: Week 3Document70 pagesSafety Management System: Week 3selcen sarıkayaPas encore d'évaluation
- Summary of What-If AnalysisDocument9 pagesSummary of What-If AnalysisjoseoliverosPas encore d'évaluation
- Human Error - in The LoopDocument3 pagesHuman Error - in The Loopsl1828Pas encore d'évaluation
- Fault Tree AnalysisDocument18 pagesFault Tree AnalysisKyle Kelly100% (1)
- Understanding Systems For Patient SafetyDocument20 pagesUnderstanding Systems For Patient Safetyhum JavedPas encore d'évaluation
- Preliminary Hazard AnalysisDocument4 pagesPreliminary Hazard AnalysisEdmundo PulidoPas encore d'évaluation
- A Model For Cryptography in Information Security: Hayfaa Abdulzahra AteeDocument3 pagesA Model For Cryptography in Information Security: Hayfaa Abdulzahra AteeerpublicationPas encore d'évaluation
- Event Tree AnalysisDocument12 pagesEvent Tree Analysisbayu_pratama_18Pas encore d'évaluation
- Sintef - About Mto-Analysis, Tripod, Sol and MortDocument12 pagesSintef - About Mto-Analysis, Tripod, Sol and Mortamal118Pas encore d'évaluation
- Investigacion Accidentes GerenciaDocument8 pagesInvestigacion Accidentes GerenciaJuan David RosalesPas encore d'évaluation
- Human Failure Capitulo 6Document34 pagesHuman Failure Capitulo 6Fernando Alberto Sanguino ArellanoPas encore d'évaluation
- AI Assignment 1Document4 pagesAI Assignment 1Abraham Onyedikachi OguduPas encore d'évaluation
- Bullemer, P. & Vernon, D., 2015. Managing Human Reliability An AbnormDocument30 pagesBullemer, P. & Vernon, D., 2015. Managing Human Reliability An Abnormdiegochivas61Pas encore d'évaluation
- A Method For Barrier-Based Incident InvestigationDocument7 pagesA Method For Barrier-Based Incident InvestigationEzatollah SalaryPas encore d'évaluation
- Contextual Risk-Based Access ControlDocument7 pagesContextual Risk-Based Access ControlSharkLaserPas encore d'évaluation
- 3.impediments o SecurityDocument16 pages3.impediments o SecurityTakudzwa MusaririPas encore d'évaluation
- Connecting The Dots - Managing The Little Things That Lead To Big AccidentsDocument15 pagesConnecting The Dots - Managing The Little Things That Lead To Big Accidentsuserscribd2011Pas encore d'évaluation
- Simulation Research MethodsDocument40 pagesSimulation Research Methodsfhanum13Pas encore d'évaluation
- Lecture Notes 5Document11 pagesLecture Notes 5lydiaqwerty1234Pas encore d'évaluation
- Human Failure Capitulo 5Document36 pagesHuman Failure Capitulo 5Fernando Alberto Sanguino ArellanoPas encore d'évaluation
- Bowtie Pro MethodologyDocument12 pagesBowtie Pro MethodologyEfari BahchevanPas encore d'évaluation
- PBKM SADFE2007 ForensicModels PDFDocument13 pagesPBKM SADFE2007 ForensicModels PDFSaicPas encore d'évaluation
- Lecture 07 Risk AnalysisDocument18 pagesLecture 07 Risk Analysisrowan mamdouhPas encore d'évaluation
- Fault Tree AnalysisDocument5 pagesFault Tree AnalysismarioetiagoPas encore d'évaluation
- Chemical Process Safety NotesDocument49 pagesChemical Process Safety NotesSujathaKs100% (2)
- Chemical Process Safety NotesDocument59 pagesChemical Process Safety NotesRishikesh AwalePas encore d'évaluation
- Selection of Incident Investigation MethodsDocument12 pagesSelection of Incident Investigation Methodsdarya2669Pas encore d'évaluation
- Investigator Name: Event Assessed: Date of Assessment: Checklist For Formal, Written Reports (See Chapter 11)Document1 pageInvestigator Name: Event Assessed: Date of Assessment: Checklist For Formal, Written Reports (See Chapter 11)Andy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of Assessment: Investigation Follow-Up Checklist Addressed? Follow-Up Issues Yes NoDocument1 pageInvestigator Name: Event Assessed: Date of Assessment: Investigation Follow-Up Checklist Addressed? Follow-Up Issues Yes NoAndy DolmanPas encore d'évaluation
- Sample Investigation Improvement Checklist Incident Investigation GuidelineDocument2 pagesSample Investigation Improvement Checklist Incident Investigation GuidelineAndy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of AssessmentDocument1 pageInvestigator Name: Event Assessed: Date of AssessmentAndy DolmanPas encore d'évaluation
- Checklist For Developing An Incident Investigation PlanDocument1 pageChecklist For Developing An Incident Investigation PlanAndy DolmanPas encore d'évaluation
- PSM Investigation Compliance Checklist Incident Investigation GuidelineDocument1 pagePSM Investigation Compliance Checklist Incident Investigation GuidelineAndy DolmanPas encore d'évaluation
- Incident InvestDocument1 pageIncident InvestAndy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineDocument1 pageInvestigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineAndy DolmanPas encore d'évaluation
- Flashback From Waste Gas Incinerator Into Air Supply Piping: Rohm and Haas Texas Inc Deer Park, TX 77536Document8 pagesFlashback From Waste Gas Incinerator Into Air Supply Piping: Rohm and Haas Texas Inc Deer Park, TX 77536Andy DolmanPas encore d'évaluation
- Quick Checklist For Investigators: Physical ItemsDocument4 pagesQuick Checklist For Investigators: Physical ItemsAndy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineDocument1 pageInvestigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineAndy DolmanPas encore d'évaluation
- Comprehensive List of CausesDocument1 pageComprehensive List of CausesAndy DolmanPas encore d'évaluation
- Sample Formal Report Outline Incident Investigation GuidelineDocument1 pageSample Formal Report Outline Incident Investigation GuidelineAndy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of AssessmentDocument1 pageInvestigator Name: Event Assessed: Date of AssessmentAndy DolmanPas encore d'évaluation
- Incident InvestDocument16 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Customize This List For Your Use. See The CCPS Guideline For Investigating Chemical InformationDocument4 pagesCustomize This List For Your Use. See The CCPS Guideline For Investigating Chemical InformationAndy DolmanPas encore d'évaluation
- Incident InvestDocument1 pageIncident InvestAndy DolmanPas encore d'évaluation
- Incident InvestDocument5 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Appendix A: Relevant OrganizationsDocument3 pagesAppendix A: Relevant OrganizationsAndy DolmanPas encore d'évaluation
- Propane Tank Flare Off in Topeka Cause and Effect Chart: (Simplified Version) 12-2-02Document2 pagesPropane Tank Flare Off in Topeka Cause and Effect Chart: (Simplified Version) 12-2-02Andy DolmanPas encore d'évaluation
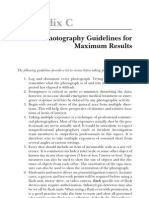
- Appendix C: Photography Guidelines For Maximum ResultsDocument3 pagesAppendix C: Photography Guidelines For Maximum ResultsAndy DolmanPas encore d'évaluation
- Appendix F: Selected OSHA and EPA Incident Investigation RegulationsDocument3 pagesAppendix F: Selected OSHA and EPA Incident Investigation RegulationsAndy DolmanPas encore d'évaluation
- Appendix B: Professional Assistance DirectoryDocument2 pagesAppendix B: Professional Assistance DirectoryAndy DolmanPas encore d'évaluation
- Incident InvestDocument21 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Checklist To Prepare For An Inspection Incident Investigation GuidelineDocument1 pageChecklist To Prepare For An Inspection Incident Investigation GuidelineAndy DolmanPas encore d'évaluation
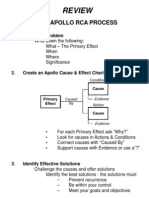
- Review: The Apollo Rca ProcessDocument1 pageReview: The Apollo Rca ProcessAndy DolmanPas encore d'évaluation
- Continuous Improvement For The Incident Investigation SystemDocument10 pagesContinuous Improvement For The Incident Investigation SystemAndy DolmanPas encore d'évaluation
- Type DG Mod 320 Part No. 952 013: Figure Without ObligationDocument1 pageType DG Mod 320 Part No. 952 013: Figure Without Obligationsherub wangdiPas encore d'évaluation
- 04 Handout 1 (Midterms)Document14 pages04 Handout 1 (Midterms)Emmanuel DelarosaPas encore d'évaluation
- Lim Resto (Perencanaan Pendirian Usaha Restaurant Fast Food)Document10 pagesLim Resto (Perencanaan Pendirian Usaha Restaurant Fast Food)Walikutay IndonesiaPas encore d'évaluation
- Welcome To Our Presentation: Submitted byDocument30 pagesWelcome To Our Presentation: Submitted byShamim MridhaPas encore d'évaluation
- Code of Ethics Multiple Choice QuestionsDocument4 pagesCode of Ethics Multiple Choice QuestionsGideon P. Casas88% (24)
- Asap 2020Document21 pagesAsap 2020KarenPas encore d'évaluation
- Allison at 500, at 1500 Series Parts Catalog: 2 1 See Section 10Document7 pagesAllison at 500, at 1500 Series Parts Catalog: 2 1 See Section 10amin chaabenPas encore d'évaluation
- Tower BridgeDocument6 pagesTower BridgeCalvin PratamaPas encore d'évaluation
- SEMIKRON DataSheet SK 30 GD 066 ET 24914960Document5 pagesSEMIKRON DataSheet SK 30 GD 066 ET 24914960prajwalPas encore d'évaluation
- DPC Clinical PaperDocument2 pagesDPC Clinical PaperAnkita KhullarPas encore d'évaluation
- HboDocument126 pagesHboKunal ChaudhryPas encore d'évaluation
- Transportation Problem 2Document11 pagesTransportation Problem 2Chasity WrightPas encore d'évaluation
- Cost Justifying HRIS InvestmentsDocument21 pagesCost Justifying HRIS InvestmentsNilesh MandlikPas encore d'évaluation
- Boat, Time Speed and DistanceDocument5 pagesBoat, Time Speed and DistanceAnmol AswalPas encore d'évaluation
- Gaps, Pro Versus NoviceDocument2 pagesGaps, Pro Versus Novicertkiyous2947Pas encore d'évaluation
- SK Memorandum of AgreementDocument3 pagesSK Memorandum of AgreementNORZEN LAGURAPas encore d'évaluation
- Is LNG Still Competitive With Other Liquid Fuels?: Proceedings, Ascope'97 ConferenceDocument18 pagesIs LNG Still Competitive With Other Liquid Fuels?: Proceedings, Ascope'97 Conferencemanolo8catalanPas encore d'évaluation
- in Re Irava Bottle ShopDocument10 pagesin Re Irava Bottle ShopCYMON KAYLE LubangcoPas encore d'évaluation
- Abstract 2 TonesDocument8 pagesAbstract 2 TonesFilip FilipovicPas encore d'évaluation
- The Ganga Pollution Cases: Mehta I (M.C. Mehta v. Union of India, (1987) 4 SCC 463)Document4 pagesThe Ganga Pollution Cases: Mehta I (M.C. Mehta v. Union of India, (1987) 4 SCC 463)SrivastavaPas encore d'évaluation
- Class 10 - Organizational Structure and CultureDocument11 pagesClass 10 - Organizational Structure and CultureTrịnh ThanhPas encore d'évaluation
- Project JavascriptDocument58 pagesProject JavascriptashwinPas encore d'évaluation
- Asus P8Z68-V PRO GEN3 ManualDocument146 pagesAsus P8Z68-V PRO GEN3 ManualwkfanPas encore d'évaluation
- 95 IDocument17 pages95 IsvishvenPas encore d'évaluation
- 12 C AdminstrationDocument2 pages12 C AdminstrationMuditPas encore d'évaluation
- Accounting QuestionsDocument16 pagesAccounting QuestionsPrachi ChananaPas encore d'évaluation
- Electrical Engineering: Scheme of Undergraduate Degree CourseDocument2 pagesElectrical Engineering: Scheme of Undergraduate Degree CourseSuresh JainPas encore d'évaluation
- Maxiim Vehicle Diagnostic ReportDocument3 pagesMaxiim Vehicle Diagnostic ReportCarlos Cobaleda GarcíaPas encore d'évaluation
- Specification For Wrought Austenitic Stainless Steel Piping FittingsDocument10 pagesSpecification For Wrought Austenitic Stainless Steel Piping FittingsAnilPas encore d'évaluation
- Advancing An Essential Clinical Data Set in Canada InfographicDocument1 pageAdvancing An Essential Clinical Data Set in Canada InfographicNICHAEL MARIA CELINA UYPas encore d'évaluation