Vous aimerez peut-être aussi
- PSM Investigation Compliance ChecklistDocument1 pagePSM Investigation Compliance ChecklistAndy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of Assessment: Checklist For Formal, Written Reports (See Chapter 11)Document1 pageInvestigator Name: Event Assessed: Date of Assessment: Checklist For Formal, Written Reports (See Chapter 11)Andy DolmanPas encore d'évaluation
- Incident InvestDocument1 pageIncident InvestAndy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineDocument1 pageInvestigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineAndy DolmanPas encore d'évaluation
- Checklist For Developing An Incident Investigation PlanDocument1 pageChecklist For Developing An Incident Investigation PlanAndy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of AssessmentDocument1 pageInvestigator Name: Event Assessed: Date of AssessmentAndy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of Assessment: Investigation Follow-Up Checklist Addressed? Follow-Up Issues Yes NoDocument1 pageInvestigator Name: Event Assessed: Date of Assessment: Investigation Follow-Up Checklist Addressed? Follow-Up Issues Yes NoAndy DolmanPas encore d'évaluation
- Sample Investigation Improvement Checklist Incident Investigation GuidelineDocument2 pagesSample Investigation Improvement Checklist Incident Investigation GuidelineAndy DolmanPas encore d'évaluation
- Customize This List For Your Use. See The CCPS Guideline For Investigating Chemical InformationDocument4 pagesCustomize This List For Your Use. See The CCPS Guideline For Investigating Chemical InformationAndy DolmanPas encore d'évaluation
- Comprehensive List of CausesDocument1 pageComprehensive List of CausesAndy DolmanPas encore d'évaluation
- Sample Formal Report Outline Incident Investigation GuidelineDocument1 pageSample Formal Report Outline Incident Investigation GuidelineAndy DolmanPas encore d'évaluation
- Quick Checklist For Investigators: Physical ItemsDocument4 pagesQuick Checklist For Investigators: Physical ItemsAndy DolmanPas encore d'évaluation
- Flashback From Waste Gas Incinerator Into Air Supply Piping: Rohm and Haas Texas Inc Deer Park, TX 77536Document8 pagesFlashback From Waste Gas Incinerator Into Air Supply Piping: Rohm and Haas Texas Inc Deer Park, TX 77536Andy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineDocument1 pageInvestigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineAndy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of AssessmentDocument1 pageInvestigator Name: Event Assessed: Date of AssessmentAndy DolmanPas encore d'évaluation
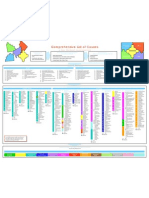
- Propane Tank Flare Off in Topeka Cause and Effect Chart: (Simplified Version) 12-2-02Document2 pagesPropane Tank Flare Off in Topeka Cause and Effect Chart: (Simplified Version) 12-2-02Andy DolmanPas encore d'évaluation
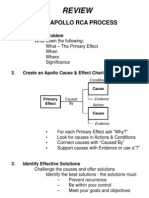
- Review: The Apollo Rca ProcessDocument1 pageReview: The Apollo Rca ProcessAndy DolmanPas encore d'évaluation
- Incident InvestDocument21 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Incident InvestDocument5 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Quick checklist for incident investigatorsDocument5 pagesQuick checklist for incident investigatorsAndy DolmanPas encore d'évaluation
- Incident InvestDocument17 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Incident InvestDocument16 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Appendix C: Photography Guidelines For Maximum ResultsDocument3 pagesAppendix C: Photography Guidelines For Maximum ResultsAndy DolmanPas encore d'évaluation
- Incident InvestDocument1 pageIncident InvestAndy DolmanPas encore d'évaluation
- Appendix F: Selected OSHA and EPA Incident Investigation RegulationsDocument3 pagesAppendix F: Selected OSHA and EPA Incident Investigation RegulationsAndy DolmanPas encore d'évaluation
- Relevant Organizations GuideDocument3 pagesRelevant Organizations GuideAndy DolmanPas encore d'évaluation
- Continuous Improvement For The Incident Investigation SystemDocument10 pagesContinuous Improvement For The Incident Investigation SystemAndy DolmanPas encore d'évaluation
- Incident InvestDocument17 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Appendix B: Professional Assistance DirectoryDocument2 pagesAppendix B: Professional Assistance DirectoryAndy DolmanPas encore d'évaluation
- Checklist To Prepare For An Inspection Incident Investigation GuidelineDocument1 pageChecklist To Prepare For An Inspection Incident Investigation GuidelineAndy DolmanPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- ATT III - 13. Prevent, Control and Fight Fires On BoardDocument9 pagesATT III - 13. Prevent, Control and Fight Fires On BoardPak WePas encore d'évaluation
- Chapter 3Document12 pagesChapter 3Raymond LeoPas encore d'évaluation
- Murat Kenedy: Bu Içerik Tarafından HazırlanmıştırDocument2 pagesMurat Kenedy: Bu Içerik Tarafından HazırlanmıştırChatorg. orgPas encore d'évaluation
- Artificial MusclesDocument8 pagesArtificial MusclespinnakapentiumPas encore d'évaluation
- Secondary SourcesDocument4 pagesSecondary SourcesKevin NgoPas encore d'évaluation
- Corporate Presentation Codex International Fev 2022Document9 pagesCorporate Presentation Codex International Fev 2022Stephane SeguierPas encore d'évaluation
- Report CategoryWiseSECCVerification 315700301009 08 2019Document2 pagesReport CategoryWiseSECCVerification 315700301009 08 2019Sandeep ChauhanPas encore d'évaluation
- Career Paralysis (PT 1) - Five Reasons Why Our Brains Get Stuck Making Career DecisionsDocument99 pagesCareer Paralysis (PT 1) - Five Reasons Why Our Brains Get Stuck Making Career DecisionsToni ErdfeldPas encore d'évaluation
- Process Strategy PPT at BEC DOMSDocument68 pagesProcess Strategy PPT at BEC DOMSBabasab Patil (Karrisatte)100% (1)
- How To Set Up Simulator Ard MMDocument12 pagesHow To Set Up Simulator Ard MMJayakrishnaPas encore d'évaluation
- Exp# 1c Exec System Call Aim: CS2257 Operating System LabDocument3 pagesExp# 1c Exec System Call Aim: CS2257 Operating System LabAbuzar ShPas encore d'évaluation
- Cylindrical Plug Gage DesignsDocument3 pagesCylindrical Plug Gage DesignskkphadnisPas encore d'évaluation
- Planets Classification Malefic and BeneficDocument3 pagesPlanets Classification Malefic and Beneficmadhu77Pas encore d'évaluation
- Mental Health Stigma and Help SeekingDocument4 pagesMental Health Stigma and Help SeekingJane Arian BerzabalPas encore d'évaluation
- Register for a WordPress account in 5 easy stepsDocument5 pagesRegister for a WordPress account in 5 easy stepsPutriPas encore d'évaluation
- BDSM - Google SearchDocument1 pageBDSM - Google SearchporcogalliardsgfPas encore d'évaluation
- Risk in Clean RoomDocument9 pagesRisk in Clean RoomABEERPas encore d'évaluation
- What Is The Procedure For Graceful Shutdown and Power Up of A Storage System During Scheduled Power OutageDocument5 pagesWhat Is The Procedure For Graceful Shutdown and Power Up of A Storage System During Scheduled Power OutageNiraj MistryPas encore d'évaluation
- Maintenance Procedure For Switchyard Equipment Volume-II (EHDocument39 pagesMaintenance Procedure For Switchyard Equipment Volume-II (EHbisas_rishiPas encore d'évaluation
- BF 00571142Document1 pageBF 00571142Tymoteusz DziedzicPas encore d'évaluation
- Regulation of AlternatorDocument6 pagesRegulation of Alternatorkudupudinagesh100% (1)
- Concept MappingDocument8 pagesConcept MappingRashid LatiefPas encore d'évaluation
- SOLID-LIQUID EXTRACTIONDocument4 pagesSOLID-LIQUID EXTRACTIONHarshal Agrawal100% (1)
- Manual de Diagnostico D3E PDFDocument72 pagesManual de Diagnostico D3E PDFJosé Luis Contreras Calderón100% (3)
- ADC MethodDocument16 pagesADC MethodPhilip K MathewPas encore d'évaluation
- Industrial Applications of Olefin MetathesisDocument7 pagesIndustrial Applications of Olefin Metathesisdogmanstar100% (1)
- Mockups Showeet (Standard)Document46 pagesMockups Showeet (Standard)Palo Alto Turismo y EntretenimientoPas encore d'évaluation
- Electrical Design Analysis: 3 Storey Commercial BuildingDocument6 pagesElectrical Design Analysis: 3 Storey Commercial Buildingcjay ganir0% (1)
- Chapter 6 THE SECOND LAW OF THERMODYNAMICS5704685Document29 pagesChapter 6 THE SECOND LAW OF THERMODYNAMICS5704685bensonPas encore d'évaluation
- McMurdo SART S4 v1 A4 06-13-2019Document2 pagesMcMurdo SART S4 v1 A4 06-13-2019Felipe OliveiraPas encore d'évaluation