Vous aimerez peut-être aussi
- What Went Wrong Issue 55Document4 pagesWhat Went Wrong Issue 55kirandevi1981Pas encore d'évaluation
- Biogas SystemsDocument8 pagesBiogas SystemsvedpathakPas encore d'évaluation
- Design Guidelines For Safety in Piping NetworkDocument15 pagesDesign Guidelines For Safety in Piping NetworkrvnesariPas encore d'évaluation
- Delay in Opening of LP Bypass ValveDocument94 pagesDelay in Opening of LP Bypass ValveCharu ChhabraPas encore d'évaluation
- The Design and Operation of Offshore Relief - Venting SystemsDocument24 pagesThe Design and Operation of Offshore Relief - Venting SystemsMichael HaisePas encore d'évaluation
- CSHS 2003 GajicDocument16 pagesCSHS 2003 GajicMircea BolovedeaPas encore d'évaluation
- Model A Deluge Valve Features and OperationDocument4 pagesModel A Deluge Valve Features and OperationmanbkkPas encore d'évaluation
- Reciprocating Compressor ValveDocument14 pagesReciprocating Compressor ValvesaikatchoudhuriPas encore d'évaluation
- Control Valves in Process PlantDocument8 pagesControl Valves in Process Plantmukramah.yusufPas encore d'évaluation
- Reduce Emissions with Proper Emission Control System MaintenanceDocument16 pagesReduce Emissions with Proper Emission Control System MaintenancevixentdPas encore d'évaluation
- Maritime Safety Valve MaintenanceDocument11 pagesMaritime Safety Valve MaintenanceAayush Agrawal100% (1)
- Design and Fabrication of Pulse Jet - ReportDocument50 pagesDesign and Fabrication of Pulse Jet - ReportVineet Jason100% (1)
- Commissioning Gas Turbine CompressorDocument13 pagesCommissioning Gas Turbine CompressorLenaldy Nuari Garnoko0% (2)
- Julian2014 PDFDocument9 pagesJulian2014 PDFmahmoud korieshPas encore d'évaluation
- AC-AIR CONDITIONING SYSTEM CIRCUIT AND COMPONENTSDocument56 pagesAC-AIR CONDITIONING SYSTEM CIRCUIT AND COMPONENTSBenjamin LarsonPas encore d'évaluation
- Simulation Based Training in Fire PDocument12 pagesSimulation Based Training in Fire Pnxyzsy4pvgPas encore d'évaluation
- Air Preheater Seal Upgrades Renew Plant EfficiencyDocument11 pagesAir Preheater Seal Upgrades Renew Plant EfficiencyN SPas encore d'évaluation
- Boiler Aalborg Aq-2 OvimuDocument193 pagesBoiler Aalborg Aq-2 Ovimunguyenvanhai1903198175% (4)
- II. In-Depth Installation Information: RestekDocument19 pagesII. In-Depth Installation Information: RestekBikas SahaPas encore d'évaluation
- Pacakage Aircon MaintenanceDocument15 pagesPacakage Aircon Maintenancerjv.premi74Pas encore d'évaluation
- APH Seal LeakagesDocument17 pagesAPH Seal LeakagesBhargav ChaudhariPas encore d'évaluation
- Of Fire In: A.K. Mukhopadhyay and P.P. SinghDocument13 pagesOf Fire In: A.K. Mukhopadhyay and P.P. SinghImmanuelPas encore d'évaluation
- Elantra 2.0 EC (137) G 2.0 MPIDocument23 pagesElantra 2.0 EC (137) G 2.0 MPIjoan velaPas encore d'évaluation
- Flare and Burn PitDocument25 pagesFlare and Burn PitHamzy Hazry100% (1)
- Chapter 9Document15 pagesChapter 9Harjith Vaibav100% (1)
- Steam EjectorsDocument6 pagesSteam EjectorsmayurjannuPas encore d'évaluation
- Understanding EjectorDocument6 pagesUnderstanding EjectormrazamudinishakPas encore d'évaluation
- Dreadnought Type 2 in 1 Brake EjectorDocument10 pagesDreadnought Type 2 in 1 Brake EjectorVikk SuriyaPas encore d'évaluation
- SDS1230 21 51 00Document30 pagesSDS1230 21 51 00นาถวัฒน์ ฉลาดแย้มPas encore d'évaluation
- Transformer Tank Rupture A Protection Engineers ChallengeDocument29 pagesTransformer Tank Rupture A Protection Engineers ChallengeJ MPas encore d'évaluation
- 2GR-FE Emission ControlDocument23 pages2GR-FE Emission ControlLuks FernandezPas encore d'évaluation
- Gas Turbine - Part 1Document82 pagesGas Turbine - Part 1Manuel L Lombardero100% (2)
- Etécnica Delugevalve ADocument16 pagesEtécnica Delugevalve Avaldemarborges6929Pas encore d'évaluation
- Yazd-System Description For Clean Drain System PDFDocument7 pagesYazd-System Description For Clean Drain System PDFace-winniePas encore d'évaluation
- 09 - Buchholz Relay - AspeDocument13 pages09 - Buchholz Relay - AspeJosé ZambranoPas encore d'évaluation
- Md1 0 V 111-09-00008 A Extraction System RequirementsDocument29 pagesMd1 0 V 111-09-00008 A Extraction System RequirementsNguyễn ĐứcPas encore d'évaluation
- Condenser Vacuum ProblemDocument4 pagesCondenser Vacuum ProblemCharu ChhabraPas encore d'évaluation
- Conventional Valves GuideDocument23 pagesConventional Valves GuidePower PlantPas encore d'évaluation
- Unit-Vi Vaporizers: Submerged Combustion Vaporizers-Open Rack Vaporizers - Shell and TubeDocument15 pagesUnit-Vi Vaporizers: Submerged Combustion Vaporizers-Open Rack Vaporizers - Shell and Tubeprathesh prasadPas encore d'évaluation
- Bottom Blowdown: Download The (295 KB) Try Answering The For This Tutorial View The Complete Collection ofDocument8 pagesBottom Blowdown: Download The (295 KB) Try Answering The For This Tutorial View The Complete Collection ofsenaPas encore d'évaluation
- Furnace 1Document73 pagesFurnace 1Volodymyr KryvetsPas encore d'évaluation
- SDS1230 21 23 00Document14 pagesSDS1230 21 23 00นาถวัฒน์ ฉลาดแย้มPas encore d'évaluation
- Idle Air Control (Iac) Valve: On-Vehicle InspectionDocument12 pagesIdle Air Control (Iac) Valve: On-Vehicle InspectionhazchuenPas encore d'évaluation
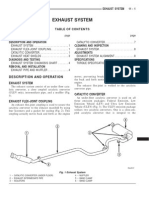
- Repair Exhaust System ComponentsDocument0 pageRepair Exhaust System ComponentstsuelectronicoPas encore d'évaluation
- Oisd CS 2021 22 P&e 03Document3 pagesOisd CS 2021 22 P&e 03Utsav DarjiPas encore d'évaluation
- A Tale of Three Pigs: Pigging Incident 1Document4 pagesA Tale of Three Pigs: Pigging Incident 1biksutong100% (1)
- 2010 Toyota Prius Repair Manual - Exhaust Heat RecirculationDocument10 pages2010 Toyota Prius Repair Manual - Exhaust Heat RecirculationMuhammad Imran Aftab100% (1)
- MIT-EL-80-017-09574615 Steam Bubble Collapse Water Hammer and Piping Network Response Volume 1 PDFDocument51 pagesMIT-EL-80-017-09574615 Steam Bubble Collapse Water Hammer and Piping Network Response Volume 1 PDFhamadaniPas encore d'évaluation
- Case Study Large Industrial Ball Valve Fire PDFDocument7 pagesCase Study Large Industrial Ball Valve Fire PDFmosptPas encore d'évaluation
- ERV Floating ProcedureDocument16 pagesERV Floating ProcedureDipti BhanjaPas encore d'évaluation
- Knowledge Management Series-Low Vacuum in Steam Turbine PDFDocument4 pagesKnowledge Management Series-Low Vacuum in Steam Turbine PDFMadhusudhan Pasumarty100% (1)
- Steam Exchanger Operation and ComponentsDocument10 pagesSteam Exchanger Operation and ComponentsMahmoud Ahmed Ali AbdelrazikPas encore d'évaluation
- Prevention of Valve Fugitive Emissions in the Oil and Gas IndustryD'EverandPrevention of Valve Fugitive Emissions in the Oil and Gas IndustryPas encore d'évaluation
- PNEUMATICS AND AIR CIRCUITS UNDERSTANDING THE CASCADE VALVE AND PLC UNDERSTANDINGD'EverandPNEUMATICS AND AIR CIRCUITS UNDERSTANDING THE CASCADE VALVE AND PLC UNDERSTANDINGPas encore d'évaluation
- Prevention of Actuator Emissions in the Oil and Gas IndustryD'EverandPrevention of Actuator Emissions in the Oil and Gas IndustryPas encore d'évaluation
- Scientific American Supplement, No. 365, December 30, 1882D'EverandScientific American Supplement, No. 365, December 30, 1882Pas encore d'évaluation
- Contemporary Anaesthetic Equipments.: An Aid for Healthcare ProfessionalsD'EverandContemporary Anaesthetic Equipments.: An Aid for Healthcare ProfessionalsPas encore d'évaluation
- Installation and Operation Instructions For Custom Mark III CP Series Oil Fired UnitD'EverandInstallation and Operation Instructions For Custom Mark III CP Series Oil Fired UnitPas encore d'évaluation
- Scientific American Supplement, No. 623, December 10, 1887D'EverandScientific American Supplement, No. 623, December 10, 1887Pas encore d'évaluation
- Incident InvestDocument1 pageIncident InvestAndy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of Assessment: Checklist For Formal, Written Reports (See Chapter 11)Document1 pageInvestigator Name: Event Assessed: Date of Assessment: Checklist For Formal, Written Reports (See Chapter 11)Andy DolmanPas encore d'évaluation
- PSM Investigation Compliance ChecklistDocument1 pagePSM Investigation Compliance ChecklistAndy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineDocument1 pageInvestigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineAndy DolmanPas encore d'évaluation
- Quick Checklist For Investigators: Physical ItemsDocument4 pagesQuick Checklist For Investigators: Physical ItemsAndy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of Assessment: Investigation Follow-Up Checklist Addressed? Follow-Up Issues Yes NoDocument1 pageInvestigator Name: Event Assessed: Date of Assessment: Investigation Follow-Up Checklist Addressed? Follow-Up Issues Yes NoAndy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of AssessmentDocument1 pageInvestigator Name: Event Assessed: Date of AssessmentAndy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineDocument1 pageInvestigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineAndy DolmanPas encore d'évaluation
- Checklist For Developing An Incident Investigation PlanDocument1 pageChecklist For Developing An Incident Investigation PlanAndy DolmanPas encore d'évaluation
- Sample Investigation Improvement Checklist Incident Investigation GuidelineDocument2 pagesSample Investigation Improvement Checklist Incident Investigation GuidelineAndy DolmanPas encore d'évaluation
- Comprehensive List of CausesDocument1 pageComprehensive List of CausesAndy DolmanPas encore d'évaluation
- Sample Formal Report Outline Incident Investigation GuidelineDocument1 pageSample Formal Report Outline Incident Investigation GuidelineAndy DolmanPas encore d'évaluation
- Appendix F: Selected OSHA and EPA Incident Investigation RegulationsDocument3 pagesAppendix F: Selected OSHA and EPA Incident Investigation RegulationsAndy DolmanPas encore d'évaluation
- Propane Tank Flare Off in Topeka Cause and Effect Chart: (Simplified Version) 12-2-02Document2 pagesPropane Tank Flare Off in Topeka Cause and Effect Chart: (Simplified Version) 12-2-02Andy DolmanPas encore d'évaluation
- Customize This List For Your Use. See The CCPS Guideline For Investigating Chemical InformationDocument4 pagesCustomize This List For Your Use. See The CCPS Guideline For Investigating Chemical InformationAndy DolmanPas encore d'évaluation
- Incident InvestDocument21 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Investigator Name: Event Assessed: Date of AssessmentDocument1 pageInvestigator Name: Event Assessed: Date of AssessmentAndy DolmanPas encore d'évaluation
- Incident InvestDocument1 pageIncident InvestAndy DolmanPas encore d'évaluation
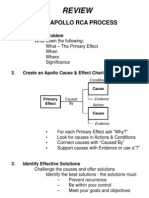
- Review: The Apollo Rca ProcessDocument1 pageReview: The Apollo Rca ProcessAndy DolmanPas encore d'évaluation
- Quick checklist for incident investigatorsDocument5 pagesQuick checklist for incident investigatorsAndy DolmanPas encore d'évaluation
- Incident InvestDocument16 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Incident InvestDocument5 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Appendix C: Photography Guidelines For Maximum ResultsDocument3 pagesAppendix C: Photography Guidelines For Maximum ResultsAndy DolmanPas encore d'évaluation
- Checklist To Prepare For An Inspection Incident Investigation GuidelineDocument1 pageChecklist To Prepare For An Inspection Incident Investigation GuidelineAndy DolmanPas encore d'évaluation
- Appendix B: Professional Assistance DirectoryDocument2 pagesAppendix B: Professional Assistance DirectoryAndy DolmanPas encore d'évaluation
- Continuous Improvement For The Incident Investigation SystemDocument10 pagesContinuous Improvement For The Incident Investigation SystemAndy DolmanPas encore d'évaluation
- Relevant Organizations GuideDocument3 pagesRelevant Organizations GuideAndy DolmanPas encore d'évaluation
- Incident InvestDocument17 pagesIncident InvestAndy DolmanPas encore d'évaluation
- Incident InvestDocument17 pagesIncident InvestAndy DolmanPas encore d'évaluation
- EMJ42003 2122S1 - Assignment 1 (Q)Document3 pagesEMJ42003 2122S1 - Assignment 1 (Q)Ishak HashimPas encore d'évaluation
- 3.5L V6 PDFDocument18 pages3.5L V6 PDFMatthew Keepin0% (1)
- Roof Insulation: Southern California Gas Company New Buildings Institute Advanced Design Guideline SeriesDocument31 pagesRoof Insulation: Southern California Gas Company New Buildings Institute Advanced Design Guideline Seriesapi-19789368100% (1)
- Practical Power System Protection - Book ReviewDocument2 pagesPractical Power System Protection - Book Reviewحمزة الفيتوريPas encore d'évaluation
- Thermal Energy Storage in Office BuildingsDocument42 pagesThermal Energy Storage in Office BuildingsnorshadiaPas encore d'évaluation
- 3-Stresses in TrackDocument49 pages3-Stresses in Trackarpit_089Pas encore d'évaluation
- Escudero, Tosh Harold Francis S.-CWTS101-BM7-PP01Document4 pagesEscudero, Tosh Harold Francis S.-CWTS101-BM7-PP01Tosh EscuderoPas encore d'évaluation
- (6600) - 4 CYL AG TRACTOR (9/75-12/81) (06E01) - OIL PUMP & PAN (SUMP) New Holland AgricultureDocument4 pages(6600) - 4 CYL AG TRACTOR (9/75-12/81) (06E01) - OIL PUMP & PAN (SUMP) New Holland AgriculturerodrigoPas encore d'évaluation
- Master Instruction for SRI986 Electro-Pneumatic PositionerDocument32 pagesMaster Instruction for SRI986 Electro-Pneumatic Positionerclebeson_pontalPas encore d'évaluation
- Dismantling of BoilerDocument2 pagesDismantling of BoilerElie ShPas encore d'évaluation
- BOQ - SIPIL GI 150 KV RAJAPAKSIDocument14 pagesBOQ - SIPIL GI 150 KV RAJAPAKSIReinhard Jesaya SimbolonPas encore d'évaluation
- ESR-Suctionpot AssemblyDocument10 pagesESR-Suctionpot Assemblybmanojkumar16Pas encore d'évaluation
- Carburetor Troubleshooting Guide: Cold Starting ProblemDocument1 pageCarburetor Troubleshooting Guide: Cold Starting ProblemhemaPas encore d'évaluation
- Ultrasonic Gas Metering Skid SpecificationDocument38 pagesUltrasonic Gas Metering Skid Specificationer_bhavin3119100% (1)
- Industrial Gas Springs: Function, Calculation and Mounting TipsDocument45 pagesIndustrial Gas Springs: Function, Calculation and Mounting TipsSavaliya HardikPas encore d'évaluation
- Short Notes On Carbon Cycle, Nitrogen Cycle and Sulphur CycleDocument16 pagesShort Notes On Carbon Cycle, Nitrogen Cycle and Sulphur Cyclesivaaero41Pas encore d'évaluation
- SK Crude Dewaxing ProcessDocument23 pagesSK Crude Dewaxing ProcessBabji MunagalaPas encore d'évaluation
- Structural Concept DesignDocument8 pagesStructural Concept DesignaahtagoPas encore d'évaluation
- Aero Indoor and Weathertight Outdoor Air Handlers: Product DataDocument172 pagesAero Indoor and Weathertight Outdoor Air Handlers: Product DataANGEL MURILLOPas encore d'évaluation
- Intelligent Building Automation SystemsDocument27 pagesIntelligent Building Automation SystemsManu Manohar0% (1)
- Installation, Operation and Maintenance Instructions: Penberthy Model Tme MixerDocument4 pagesInstallation, Operation and Maintenance Instructions: Penberthy Model Tme MixerGuillermo MartinezPas encore d'évaluation
- Komatsu D85 A-21 Crawler Tractor PDFDocument2 pagesKomatsu D85 A-21 Crawler Tractor PDFrandy patah asbiPas encore d'évaluation
- Safety EN IEC 60335 1 Cyrix PDFDocument106 pagesSafety EN IEC 60335 1 Cyrix PDFGiuseppe FerrariPas encore d'évaluation
- Sky Air Seasonal Classic Conductos Baja Silueta Serie DDocument1 pageSky Air Seasonal Classic Conductos Baja Silueta Serie DmiroPas encore d'évaluation
- 1A Low Dropout Linear Regulator: General DescriptionDocument11 pages1A Low Dropout Linear Regulator: General DescriptionTito NavarroPas encore d'évaluation
- Journal of Molecular Liquids: Mohammad Hatami Maryam Hasanpour, Dengwei JingDocument22 pagesJournal of Molecular Liquids: Mohammad Hatami Maryam Hasanpour, Dengwei JingSugam KarkiPas encore d'évaluation
- Energy Revision Summary Key PointsDocument8 pagesEnergy Revision Summary Key PointsyuhPas encore d'évaluation
- API Monogram Products: SelectDocument4 pagesAPI Monogram Products: SelectvsantenrPas encore d'évaluation
- ClassNK - MEPC80 SummaryDocument5 pagesClassNK - MEPC80 SummaryPereira JenPas encore d'évaluation
- IRA-4SS Automatic Insertion Instrument Regulator: Engineering CompanyDocument2 pagesIRA-4SS Automatic Insertion Instrument Regulator: Engineering CompanyRuben Ortiz CaramPas encore d'évaluation