Vous aimerez peut-être aussi
- Supplies and Reagents:: Serum ELISA Rev 07-18Document1 pageSupplies and Reagents:: Serum ELISA Rev 07-18umairas_1Pas encore d'évaluation
- Physics Form 4 NotesDocument97 pagesPhysics Form 4 Notesumairas_1Pas encore d'évaluation
- Physics Form 4 NotesDocument97 pagesPhysics Form 4 Notesumairas_1Pas encore d'évaluation
- Nerves, Hormones and HomeostasisDocument8 pagesNerves, Hormones and Homeostasisumairas_1Pas encore d'évaluation
- Complementry and Alternative Medicine: History, Definitions, and What Is It Today?Document38 pagesComplementry and Alternative Medicine: History, Definitions, and What Is It Today?umairas_1Pas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- NCP PcapDocument1 pageNCP PcapLhexie CooperPas encore d'évaluation
- 52 Healing HabitsDocument11 pages52 Healing Habitsjethro123_69Pas encore d'évaluation
- Venipunture ProcedureDocument4 pagesVenipunture ProcedureAnusha VerghesePas encore d'évaluation
- Drug DetoxcificationDocument23 pagesDrug DetoxcificationPUSAT LATIHAN AADKPas encore d'évaluation
- Liver Ki GarmiDocument8 pagesLiver Ki GarmidineshPas encore d'évaluation
- Factors Influencing Health and HDDocument22 pagesFactors Influencing Health and HDapi-311270394Pas encore d'évaluation
- Secondary Angle Closure GlaucomaDocument35 pagesSecondary Angle Closure GlaucomaAndriati NadhilaPas encore d'évaluation
- Satara ODF ReportDocument27 pagesSatara ODF ReportPrashant JadhavPas encore d'évaluation
- Fracasso - Energy Medicine 2010Document39 pagesFracasso - Energy Medicine 2010api-308577129100% (1)
- Decup 2014Document8 pagesDecup 2014Elija BrockPas encore d'évaluation
- 120276533-WMOGT-5th April-2013Document2 pages120276533-WMOGT-5th April-2013wmogtPas encore d'évaluation
- Video Game TreatmentDocument1 pageVideo Game TreatmentYosi FestaPas encore d'évaluation
- Hypertension CASE STUDYDocument30 pagesHypertension CASE STUDYKaloy Kamao100% (7)
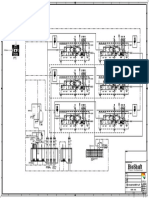
- P&ID - STP-Yanbu SWCC (6units)Document1 pageP&ID - STP-Yanbu SWCC (6units)Ashraf BayomiPas encore d'évaluation
- Vicky Sawyer: Misusing and Abusing 'Science' in The Cause of Transgenderism and HomosexualityDocument4 pagesVicky Sawyer: Misusing and Abusing 'Science' in The Cause of Transgenderism and HomosexualityRogerWilliamsPas encore d'évaluation
- Pharmacology Table For Cardiovascular LectureDocument10 pagesPharmacology Table For Cardiovascular LecturemuhammadridhwanPas encore d'évaluation
- CWS Lagoons MBR SystemsDocument3 pagesCWS Lagoons MBR SystemsZoran DespotovicPas encore d'évaluation
- TTS 16 80 400 Septic Tank DesingsDocument16 pagesTTS 16 80 400 Septic Tank DesingsJeffrey James100% (2)
- Antibiotics ChartDocument10 pagesAntibiotics Chartadom09Pas encore d'évaluation
- South West Regional Bulletin: A Message From The Director All Change at The CentreDocument19 pagesSouth West Regional Bulletin: A Message From The Director All Change at The Centre433188Pas encore d'évaluation
- Neal Sal Z Testimonials OnDocument6 pagesNeal Sal Z Testimonials OnCarlos LiraPas encore d'évaluation
- Daftar Obat High Alert MedicationDocument7 pagesDaftar Obat High Alert Medicationlala bestgirlPas encore d'évaluation
- Design, Development and Evaluation of Econazole Nitrate Emulgel For Topical Fungal DiseaseDocument18 pagesDesign, Development and Evaluation of Econazole Nitrate Emulgel For Topical Fungal DiseaseIhsanti Dwi RahayuPas encore d'évaluation
- What Are The Benefits of An Intensive Outpatient ProgramDocument2 pagesWhat Are The Benefits of An Intensive Outpatient ProgramDan MarkPas encore d'évaluation
- Dr. Suryono, SPJPDocument26 pagesDr. Suryono, SPJPPowool LalaPas encore d'évaluation
- Act For Insomnia Act I by DR Guy Meadows The Sleep SchoolDocument7 pagesAct For Insomnia Act I by DR Guy Meadows The Sleep SchoolDharmendra KumarPas encore d'évaluation
- ADHD and Self EfficacyDocument20 pagesADHD and Self Efficacygeorgianaberariu6758Pas encore d'évaluation
- Lab 1 - Asepsis and Infection Control QuestionsDocument3 pagesLab 1 - Asepsis and Infection Control QuestionsmlomiguenPas encore d'évaluation
- Emphasis On Non-Pharmacologic Aspect: Key Principles: o Gate Control & Neuromatrix Theory of PainDocument3 pagesEmphasis On Non-Pharmacologic Aspect: Key Principles: o Gate Control & Neuromatrix Theory of PainJudy Ignacio EclarinoPas encore d'évaluation
- Yakeley 2018 Psychoanalysis in Modern Mental Health PracticeDocument8 pagesYakeley 2018 Psychoanalysis in Modern Mental Health PracticeJonathan RiveraPas encore d'évaluation