Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Aircraft Instrument MaintenanceDocument22 pagesAircraft Instrument MaintenanceBharath Kumar Goud83% (6)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Standard For Fibre Reinforced Plastic Underground Tanks For Flammable and Combustible LiquidsDocument38 pagesStandard For Fibre Reinforced Plastic Underground Tanks For Flammable and Combustible Liquidsgrincheu70Pas encore d'évaluation
- CoCom Lists - 1985Document68 pagesCoCom Lists - 1985Samuel EvansPas encore d'évaluation
- Astm 471Document6 pagesAstm 471JOSEPH REFUERZOPas encore d'évaluation
- Thomas 1240Document8 pagesThomas 1240maeq20080% (1)
- Helium Leak Testing Fundamentals and ApplicationsDocument21 pagesHelium Leak Testing Fundamentals and ApplicationsSaut Maruli Tua Samosir100% (1)
- 2010 IPM Day Metrics KerznerDocument53 pages2010 IPM Day Metrics KerznergpssafetyPas encore d'évaluation
- SECTION 5.40: Crankcase Breather SystemDocument24 pagesSECTION 5.40: Crankcase Breather SystemLUISA FERNANDA TORRES MANOSALVAPas encore d'évaluation
- Overview On Ash Handling SystemDocument58 pagesOverview On Ash Handling SystemDebkumar958Pas encore d'évaluation
- Calibrating a Pressure Gauge and Calculating ErrorDocument3 pagesCalibrating a Pressure Gauge and Calculating Error047-Nidhi HingankarPas encore d'évaluation
- Godwin Cd150m Parts ListDocument2 pagesGodwin Cd150m Parts ListJenni33% (3)
- Vessel Particulars Questionnaire For Bulk Oil/Chemical CarriersDocument39 pagesVessel Particulars Questionnaire For Bulk Oil/Chemical CarriersjohnEnglish50% (4)
- ISO 22000 Tool - 5-04Document4 pagesISO 22000 Tool - 5-04CostasKPas encore d'évaluation
- The Dangers of Hydrogen Sulphide in Marine BunkersDocument2 pagesThe Dangers of Hydrogen Sulphide in Marine BunkersCostasKPas encore d'évaluation
- Mars 238Document6 pagesMars 238CostasKPas encore d'évaluation
- Shipping KPI Standard V20Document144 pagesShipping KPI Standard V20Desi Daneva100% (2)
- Mars 240Document4 pagesMars 240CostasKPas encore d'évaluation
- Paris MoU Preliminary Report For CIC On Fire SafetyDocument3 pagesParis MoU Preliminary Report For CIC On Fire SafetyCostasKPas encore d'évaluation
- Mars 239Document6 pagesMars 239CostasKPas encore d'évaluation
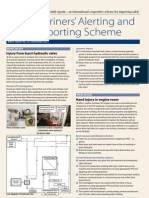
- Mariners' Alerting and Reporting Scheme: Injury From Burst Hydraulic ValveDocument4 pagesMariners' Alerting and Reporting Scheme: Injury From Burst Hydraulic ValveCostasKPas encore d'évaluation
- Mars 243Document4 pagesMars 243CostasKPas encore d'évaluation
- Continental Industrial PDFDocument359 pagesContinental Industrial PDFDavidPas encore d'évaluation
- Bloomden Milling Machine X5 Operation ManualDocument21 pagesBloomden Milling Machine X5 Operation ManualAngel TrujilloPas encore d'évaluation
- DescriptionDocument39 pagesDescriptionpritikhedekar023Pas encore d'évaluation
- Aspects of Lead Acid Battery Technology 5 Dry Charging of Formed Negative PlatesDocument12 pagesAspects of Lead Acid Battery Technology 5 Dry Charging of Formed Negative PlatestjkiddPas encore d'évaluation
- MANKENBERG - Vacuum Valve PDFDocument10 pagesMANKENBERG - Vacuum Valve PDFmikeswordsPas encore d'évaluation
- Manual Kit Rna ExtractionDocument28 pagesManual Kit Rna ExtractionNurul Syamimi OthmanPas encore d'évaluation
- Tri-Tech Vacuum SystemsDocument4 pagesTri-Tech Vacuum SystemsBebeqReebekPas encore d'évaluation
- 18 Ac79d1 8 enDocument28 pages18 Ac79d1 8 enHoàngViệtAnhPas encore d'évaluation
- Im 5 201 Us PDFDocument20 pagesIm 5 201 Us PDFCarlos Rafael Pereyra SegoviaPas encore d'évaluation
- Surface Condenser Eng2Document5 pagesSurface Condenser Eng2MuhammadFikriPas encore d'évaluation
- Astm D5191Document5 pagesAstm D5191pefevagoPas encore d'évaluation
- Oil Pump Type Ta: For Fuel Oil #2 To #6 ApplicationsDocument2 pagesOil Pump Type Ta: For Fuel Oil #2 To #6 Applicationsmochammad RezaPas encore d'évaluation
- Instuctions of Use The Resin ImpResin90 To The Wood Stabilization ProcessDocument2 pagesInstuctions of Use The Resin ImpResin90 To The Wood Stabilization ProcessjuaaltaPas encore d'évaluation
- TD Pmo 6000 en 080108Document16 pagesTD Pmo 6000 en 080108Ricardo DávilaPas encore d'évaluation
- Manual Servicio Mini Split 36Document80 pagesManual Servicio Mini Split 36Fredy Alvarado RodriguezPas encore d'évaluation
- Metrology: By: Luiz Angelo L. VillegasDocument53 pagesMetrology: By: Luiz Angelo L. VillegasLouie Ludeña VillegasPas encore d'évaluation
- Select the Right Vacuum Pump FluidDocument3 pagesSelect the Right Vacuum Pump Fluidlaraujo76Pas encore d'évaluation
- Service Manual: Seer21 Split UnitDocument102 pagesService Manual: Seer21 Split UnitGabriel GuerreroPas encore d'évaluation
- Service Manual PAC9037 PDFDocument44 pagesService Manual PAC9037 PDFinigonenoPas encore d'évaluation
- Masport Manual H HXLDocument47 pagesMasport Manual H HXLMichael Rice100% (1)