Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- ISO 22000 Tool - 5-04Document4 pagesISO 22000 Tool - 5-04CostasKPas encore d'évaluation
- 2010 IPM Day Metrics KerznerDocument53 pages2010 IPM Day Metrics KerznergpssafetyPas encore d'évaluation
- Paris MoU Preliminary Report For CIC On Fire SafetyDocument3 pagesParis MoU Preliminary Report For CIC On Fire SafetyCostasKPas encore d'évaluation
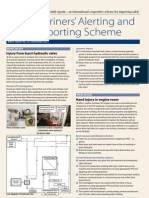
- Mariners' Alerting and Reporting Scheme: Injury From Burst Hydraulic ValveDocument4 pagesMariners' Alerting and Reporting Scheme: Injury From Burst Hydraulic ValveCostasKPas encore d'évaluation
- Mars 243Document4 pagesMars 243CostasKPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hydrometeorological Hazard StudentDocument26 pagesHydrometeorological Hazard StudentMargaret Nicole100% (1)
- Tle-Afa-Agri Crop Production: Quarter 1 - Module 5: Occupational Health and Safety Measures in The WorkplaceDocument24 pagesTle-Afa-Agri Crop Production: Quarter 1 - Module 5: Occupational Health and Safety Measures in The Workplacesheynie penalosa100% (3)
- Cara Generic TemplateDocument6 pagesCara Generic Templateapi-287145463Pas encore d'évaluation
- 5 - Risk AssessmentDocument8 pages5 - Risk AssessmentAldrien CabintePas encore d'évaluation
- Building Design For Homeland Security: Risk Management SeriesDocument159 pagesBuilding Design For Homeland Security: Risk Management Seriescklcon100% (1)
- NSP 007 002 Guidance On Substation Design - Design Risk Assessment - PDF - 0Document19 pagesNSP 007 002 Guidance On Substation Design - Design Risk Assessment - PDF - 0Kishore100% (1)
- CEP Magazine 2023 1691466815Document6 pagesCEP Magazine 2023 1691466815SameerPas encore d'évaluation
- 1.5T Express Coil Suite Operator Manual Direction 5343815-2EN Rev 6Document37 pages1.5T Express Coil Suite Operator Manual Direction 5343815-2EN Rev 6service iyadMedicalPas encore d'évaluation
- Iasimp Qs005 en PDocument200 pagesIasimp Qs005 en PIng Capriel CaprielPas encore d'évaluation
- DRRR Midterms ReviewerDocument16 pagesDRRR Midterms ReviewerHans Matthew AntiojoPas encore d'évaluation
- Getting To Grips With FDADocument84 pagesGetting To Grips With FDATanishq VashisthPas encore d'évaluation
- DRRR q3 Mod.1 4 DisasterDocument26 pagesDRRR q3 Mod.1 4 DisasterMariel Joy HernandezPas encore d'évaluation
- JSA HEMP Well Services Pg25-30Document5 pagesJSA HEMP Well Services Pg25-30Ashok SureshPas encore d'évaluation
- DRRR L3Document1 pageDRRR L3lucy brinePas encore d'évaluation
- Operating Manual: Moisture Measuring DeviceDocument8 pagesOperating Manual: Moisture Measuring DeviceCristian BujorPas encore d'évaluation
- Accident Investigation and ReportingDocument27 pagesAccident Investigation and ReportingVenkadesh PeriathambiPas encore d'évaluation
- Excavation Risk AssessmentDocument11 pagesExcavation Risk AssessmentMarwan NazzalPas encore d'évaluation
- Final 2023 SGLGB Form 1 Documentary ChecklistDocument12 pagesFinal 2023 SGLGB Form 1 Documentary ChecklistBarangay Taguitic92% (12)
- TR Rigid Off-Highway Dump Truck NC IIDocument76 pagesTR Rigid Off-Highway Dump Truck NC IIAljon Fortaleza BalanagPas encore d'évaluation
- Fire Risk Assessment-Computer SainsDocument81 pagesFire Risk Assessment-Computer SainsMuhammad IqbalPas encore d'évaluation
- Climate Risk and Response in Asia PDFDocument156 pagesClimate Risk and Response in Asia PDFPratip BhattacharyaPas encore d'évaluation
- Participatory Approach For Safe Shelter Awareness (PASSA) ManualDocument134 pagesParticipatory Approach For Safe Shelter Awareness (PASSA) ManualInternational Federation of Red Cross Red Crescent Societies (IFRC)100% (2)
- Komatsu Dump Truck Hm350 1 Operation Maintenance ManualDocument20 pagesKomatsu Dump Truck Hm350 1 Operation Maintenance Manuallydia100% (39)
- RCA2 ImprovingRootCauseAnalysesandActionstoPreventHarmDocument51 pagesRCA2 ImprovingRootCauseAnalysesandActionstoPreventHarmalejandromfunes1749Pas encore d'évaluation
- Local Shelter Plan 2018-2026: Santa Rita PampangaDocument38 pagesLocal Shelter Plan 2018-2026: Santa Rita PampangaELIAS BUENAVENTEPas encore d'évaluation
- DOH Orientation On PSCP - Public VersionDocument119 pagesDOH Orientation On PSCP - Public VersionNursing Staff Development Dr. PJGMRMCPas encore d'évaluation
- 2024 OCD5 DepEd TemplateDocument27 pages2024 OCD5 DepEd Templatemichaeljohnranada1987Pas encore d'évaluation
- WHS-42 Safe Operation of Overhead Cranes Procedure1 PDFDocument16 pagesWHS-42 Safe Operation of Overhead Cranes Procedure1 PDFviniciusgdelimaPas encore d'évaluation
- Risk Assessment ManualDocument45 pagesRisk Assessment ManualGamalMahran100% (1)
- Posters1 23 PDFDocument24 pagesPosters1 23 PDFStarius StalkerPas encore d'évaluation