Vous aimerez peut-être aussi
- End-of-Life Choices: CPR & DNR WHEN PATIENT & FAMILY CONFLICT OVER DECISION: Ethical Considerations For The Competent PatientDocument41 pagesEnd-of-Life Choices: CPR & DNR WHEN PATIENT & FAMILY CONFLICT OVER DECISION: Ethical Considerations For The Competent PatientDr. Liza ManaloPas encore d'évaluation
- PHYSICIAN Patient RelationshipDocument2 pagesPHYSICIAN Patient RelationshipRem AlfelorPas encore d'évaluation
- The Doctor Patient Relationship PDFDocument8 pagesThe Doctor Patient Relationship PDFWagiono Suparan100% (2)
- 6 Doctor Patient Relationship For Batch 18Document36 pages6 Doctor Patient Relationship For Batch 18Muhammad Sukri JafarPas encore d'évaluation
- Tvl-Fbs-11-12-Q-4-Week 6Document8 pagesTvl-Fbs-11-12-Q-4-Week 6Geh Deng NolealPas encore d'évaluation
- VariationsDocument3 pagesVariationsPasli Ismail100% (3)
- To ICT: By: Alliah Vance O. Capuz 11 Abm A-St. SebastianDocument16 pagesTo ICT: By: Alliah Vance O. Capuz 11 Abm A-St. SebastianAlliah Vance O. CapuzPas encore d'évaluation
- Doctor Patient CommunicationDocument16 pagesDoctor Patient CommunicationRobby100% (1)
- Oral Communication Midterm ReviewerDocument3 pagesOral Communication Midterm ReviewerPatrick RamirezPas encore d'évaluation
- ISO 19650 4 Exec Brief FINALDocument11 pagesISO 19650 4 Exec Brief FINALmohammad loai sabbaghPas encore d'évaluation
- 79-02 Closing The Gap Information Models in Contemporary Design PracticeDocument147 pages79-02 Closing The Gap Information Models in Contemporary Design Practiceeribeto100% (1)
- Mil DLL Week6Document3 pagesMil DLL Week6Ian JunioPas encore d'évaluation
- The Enduring and Evolving Nature of The Patient-PhysicianDocument11 pagesThe Enduring and Evolving Nature of The Patient-PhysicianSYLVIA RAMIS ASENJOPas encore d'évaluation
- Paper Salud FamiliarDocument16 pagesPaper Salud FamiliarLucas Braga Almeida e SilvaPas encore d'évaluation
- Prabavathi.u Inter-Relation Between Clinical Name ChangedDocument63 pagesPrabavathi.u Inter-Relation Between Clinical Name ChangedVenkatram PrabhuPas encore d'évaluation
- Impact of Nurse-Patient Relationship On Quality of Care and Patient Autonomy in Decision-MakingDocument24 pagesImpact of Nurse-Patient Relationship On Quality of Care and Patient Autonomy in Decision-MakingMary LowryPas encore d'évaluation
- Tugas BHP Hub Pasien DokterDocument14 pagesTugas BHP Hub Pasien DokterJoelPas encore d'évaluation
- Damodaram Sanjivayya National Law University, Nyayaprastha, Sabbavaram, Visakhapatnam, Andhra Pradesh-531035Document20 pagesDamodaram Sanjivayya National Law University, Nyayaprastha, Sabbavaram, Visakhapatnam, Andhra Pradesh-531035LegendPas encore d'évaluation
- Doctor-Patient Relationship: "A Research Assignment - Mohamed Abdulhafeez"Document6 pagesDoctor-Patient Relationship: "A Research Assignment - Mohamed Abdulhafeez"AmiiinPas encore d'évaluation
- Doctor-Patient Communication A ReviewDocument6 pagesDoctor-Patient Communication A ReviewWagiono SuparanPas encore d'évaluation
- City Research Online: City, University of London Institutional RepositoryDocument32 pagesCity Research Online: City, University of London Institutional RepositoryasadlaariPas encore d'évaluation
- Doctor Patient RelationshipDocument4 pagesDoctor Patient RelationshipvishnuPas encore d'évaluation
- Doctor-Patient Communication: A Review of The LiteratureDocument16 pagesDoctor-Patient Communication: A Review of The LiteraturenutoPas encore d'évaluation
- The Doctor-Patient RelationshipDocument9 pagesThe Doctor-Patient RelationshipAntu Chowdhury100% (1)
- STL11 2P - Doctors Interpersonal Skills - 114025Document23 pagesSTL11 2P - Doctors Interpersonal Skills - 114025pyong jPas encore d'évaluation
- Doctor-Patient Communication: A ReviewDocument8 pagesDoctor-Patient Communication: A ReviewJAKE BENZYN TEPas encore d'évaluation
- The Doctor-Patient RelationshipDocument55 pagesThe Doctor-Patient RelationshipMuhammad NaveedPas encore d'évaluation
- Street 2009 How Does Communiction HealDocument7 pagesStreet 2009 How Does Communiction HealBegert JamesPas encore d'évaluation
- Modelos de Rel M P Ezequiel 1992Document14 pagesModelos de Rel M P Ezequiel 1992carmenPas encore d'évaluation
- CPE5 AppendicesDocument55 pagesCPE5 Appendicescosmindudu1980Pas encore d'évaluation
- Doctor Patient Communication: Yasir Irafat GROUP: 11 4 Semester Submitted To: Svetlana AbdikaimovaDocument14 pagesDoctor Patient Communication: Yasir Irafat GROUP: 11 4 Semester Submitted To: Svetlana AbdikaimovaYasir IrafatPas encore d'évaluation
- Ab 2 DPR Trust Com LudwigDocument2 pagesAb 2 DPR Trust Com Ludwigapi-610178988Pas encore d'évaluation
- Kelly 2019Document10 pagesKelly 2019Siti MinartiPas encore d'évaluation
- PT CommunicationDocument4 pagesPT CommunicationdocbinPas encore d'évaluation
- Unit 3 Final DraftDocument13 pagesUnit 3 Final Draftapi-252312023Pas encore d'évaluation
- Ethical Issues in Healthcare ManagementDocument44 pagesEthical Issues in Healthcare ManagementTravel with NiroPas encore d'évaluation
- Revised ThesisDocument27 pagesRevised ThesisAira FrancescaPas encore d'évaluation
- Pharmacists and CommunicationDocument5 pagesPharmacists and CommunicationMichael BonettPas encore d'évaluation
- 11.perception of Risk and CommunicationDocument14 pages11.perception of Risk and Communicationbunga mawarPas encore d'évaluation
- Topic 3Document15 pagesTopic 3Official GBEPas encore d'évaluation
- Facilitating Rapport Through Real Patient Encounters in Health Care Professional EducationDocument8 pagesFacilitating Rapport Through Real Patient Encounters in Health Care Professional EducationLen meloPas encore d'évaluation
- A Medical Director's Perspective: Understanding The Physician PerspectiveDocument3 pagesA Medical Director's Perspective: Understanding The Physician Perspectiveacma2010Pas encore d'évaluation
- Doctor Patient Communication Literature ReviewDocument6 pagesDoctor Patient Communication Literature Reviewaflsvagfb100% (1)
- 22Document12 pages22Macarena Cortes CarvalloPas encore d'évaluation
- The Practitioners Handbook To Patient Communication From Theory To Practice: The Practitioners Handbook To Patient Communication From Theory To Practice, #1D'EverandThe Practitioners Handbook To Patient Communication From Theory To Practice: The Practitioners Handbook To Patient Communication From Theory To Practice, #1Pas encore d'évaluation
- Continuity of Care: Literature Review and ImplicationsDocument10 pagesContinuity of Care: Literature Review and ImplicationsRona RihadahPas encore d'évaluation
- Barriers in CommunicationDocument1 pageBarriers in CommunicationAfifa Noori SiddiquiPas encore d'évaluation
- Interventions To Enhance Communication Among Patients, Providers, and FamiliesDocument8 pagesInterventions To Enhance Communication Among Patients, Providers, and FamiliesvabcunhaPas encore d'évaluation
- Enc 2135 Research PaperDocument12 pagesEnc 2135 Research Paperapi-315614504100% (1)
- Jurnal 1 PDFDocument8 pagesJurnal 1 PDFDhyan Hardiyanti BaharPas encore d'évaluation
- Q1: Define Medical Sociology and Its Scope: Medical SociologyDocument2 pagesQ1: Define Medical Sociology and Its Scope: Medical Sociologyhina rasoolPas encore d'évaluation
- 18.doctor-Patient Communication and Cancer Patients' Quality of Life and SatisfactionDocument8 pages18.doctor-Patient Communication and Cancer Patients' Quality of Life and SatisfactionNia AnggreniPas encore d'évaluation
- Actitudes Tutor ClinicoDocument3 pagesActitudes Tutor Clinicoiguija6769Pas encore d'évaluation
- Approach To The Patient - UpToDateDocument35 pagesApproach To The Patient - UpToDateAmrutesh KhodkePas encore d'évaluation
- 2020 Article 742Document38 pages2020 Article 742Ratih puspita DewiPas encore d'évaluation
- Ohtaki FamPract03Document7 pagesOhtaki FamPract03mahsa moosazadehPas encore d'évaluation
- Doctor Pateint RelationshipDocument4 pagesDoctor Pateint RelationshipBhatti LrbPas encore d'évaluation
- Doctor-Patient Relationship - Cultural Aspects and Other Issues - Adel Adly RaghebDocument10 pagesDoctor-Patient Relationship - Cultural Aspects and Other Issues - Adel Adly RaghebAdel AdlyPas encore d'évaluation
- Challenges and Strategies in Caring For PhysicianDocument5 pagesChallenges and Strategies in Caring For PhysicianLuke FlemmingsPas encore d'évaluation
- CPC CornerDocument5 pagesCPC Cornereduardo perez ramirezPas encore d'évaluation
- Running Head: Literature ReviewDocument5 pagesRunning Head: Literature ReviewBrandy SangurahPas encore d'évaluation
- Article 5Document8 pagesArticle 5Purvesh PatelPas encore d'évaluation
- Research Proposal 1.1 Background of The StudyDocument9 pagesResearch Proposal 1.1 Background of The StudyFranklin GodshandPas encore d'évaluation
- The Doctor As Parent, Partner, Provider or Comrade? Distribution of Power in Past and Present Models of The Doctor-Patient RelationshipDocument18 pagesThe Doctor As Parent, Partner, Provider or Comrade? Distribution of Power in Past and Present Models of The Doctor-Patient RelationshipJuliana Tiemi SuguitaPas encore d'évaluation
- Profesionalismo MedicoDocument15 pagesProfesionalismo MedicoR4pT0r666Pas encore d'évaluation
- Journal Pone 0094207Document7 pagesJournal Pone 0094207JuanaPas encore d'évaluation
- Winner's CertificateDocument1 pageWinner's CertificateNataliya PiletskaPas encore d'évaluation
- Fluid ResuscitationDocument27 pagesFluid ResuscitationNataliya PiletskaPas encore d'évaluation
- Airway Management For ParamedicsDocument53 pagesAirway Management For ParamedicsNataliya PiletskaPas encore d'évaluation
- 70 Adrenergic NeurotransmissionDocument1 page70 Adrenergic NeurotransmissionNataliya PiletskaPas encore d'évaluation
- Sc04 L04 Gaseous Diffusion and Transport 2Document9 pagesSc04 L04 Gaseous Diffusion and Transport 2Nataliya PiletskaPas encore d'évaluation
- Taylor Swift - Reputation (Digital Booklet)Document6 pagesTaylor Swift - Reputation (Digital Booklet)lulisayisPas encore d'évaluation
- CCCU LSC BABS MM Report Nov 2023Document15 pagesCCCU LSC BABS MM Report Nov 2023MariaRaduPas encore d'évaluation
- Forensics - Manager July 09Document2 pagesForensics - Manager July 09nash666Pas encore d'évaluation
- Tenderresponse Carrier Edi990Document17 pagesTenderresponse Carrier Edi990mohamed-mofPas encore d'évaluation
- Haapio, 2014, DLDocument8 pagesHaapio, 2014, DLnecroticvsPas encore d'évaluation
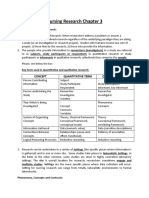
- Nursing Research Chapter 3: The Building Blocks of ResearchDocument4 pagesNursing Research Chapter 3: The Building Blocks of ResearchSupriadi74Pas encore d'évaluation
- Assessment 1 - How To Pay A Pizza Shop Telephone OperatorDocument4 pagesAssessment 1 - How To Pay A Pizza Shop Telephone OperatorJulian BrownPas encore d'évaluation
- Thesis Operational Risk ManagementDocument7 pagesThesis Operational Risk Managementjenniferwatsonmobile100% (2)
- Group 24 ReportDocument48 pagesGroup 24 ReportVishwanath GroupsPas encore d'évaluation
- Online Travel Order Processing System Release 4 User's ManualDocument32 pagesOnline Travel Order Processing System Release 4 User's ManualRichard AdrianPas encore d'évaluation
- Ges 107 Note 2022Document61 pagesGes 107 Note 2022Abdullah Onisabi100% (1)
- Scheduling System Thesis SampleDocument7 pagesScheduling System Thesis Sampleeifvhpugg100% (2)
- Information Analysis Project (IAP) : ObjectivesDocument3 pagesInformation Analysis Project (IAP) : ObjectivesIsaiah BatucanPas encore d'évaluation
- BlahtDocument14 pagesBlahtjessa mae zerdaPas encore d'évaluation
- Cefr - Speaking (Year 1 and 2)Document2 pagesCefr - Speaking (Year 1 and 2)Tan S YeePas encore d'évaluation
- Essay 2Document2 pagesEssay 2akuramlan1978Pas encore d'évaluation
- OMAXDocument28 pagesOMAXAlisa KobzarPas encore d'évaluation
- Roll No. 107 Rajvardhan Singh SolankiDocument2 pagesRoll No. 107 Rajvardhan Singh SolankiSurya pratap SinghPas encore d'évaluation
- Cagayan State University - College of Information TechnologyDocument26 pagesCagayan State University - College of Information TechnologyChristian Pasicolan50% (2)
- Wati Assessment PackageDocument22 pagesWati Assessment Packageapi-284405648Pas encore d'évaluation
- Junior Research Analyst - 20110704Document10 pagesJunior Research Analyst - 20110704Rebel_DragonPas encore d'évaluation
- CSTA K-12 Standards Progression ChartDocument2 pagesCSTA K-12 Standards Progression ChartBryan TwarekPas encore d'évaluation
- Chapter One I.1 Background To The StudyDocument81 pagesChapter One I.1 Background To The StudyRathin BanerjeePas encore d'évaluation