Vous aimerez peut-être aussi
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- 11-Car ModelsDocument27 pages11-Car ModelsNiong DavidPas encore d'évaluation
- Principles of Exterior DrainageDocument60 pagesPrinciples of Exterior DrainageSeshupower09Pas encore d'évaluation
- Aurora Model 481 Pumps: Single-Stage Fire ServiceDocument1 pageAurora Model 481 Pumps: Single-Stage Fire ServiceNiong DavidPas encore d'évaluation
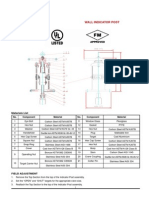
- 6 Rel-Pi-Wall Indicator PostDocument1 page6 Rel-Pi-Wall Indicator PostNiong DavidPas encore d'évaluation
- 08 08.pump Station - IfbDocument35 pages08 08.pump Station - IfbNiong DavidPas encore d'évaluation
- Articles - Elevator Car SizesDocument5 pagesArticles - Elevator Car SizesNiong DavidPas encore d'évaluation
- Electrical EngineeringElevator Safety SystemDocument13 pagesElectrical EngineeringElevator Safety SystemNiong DavidPas encore d'évaluation
- Compressed Air Ref EngDocument118 pagesCompressed Air Ref Engchidambaram kasiPas encore d'évaluation
- FMDS0404NDocument5 pagesFMDS0404NStory LovePas encore d'évaluation
- Basic Elevator Components - Part OneDocument16 pagesBasic Elevator Components - Part OneNiong DavidPas encore d'évaluation
- PSD Ceu 198april13Document16 pagesPSD Ceu 198april13Niong DavidPas encore d'évaluation
- Manual 10 - Irrigation Scheme Operation and MaintenanceDocument55 pagesManual 10 - Irrigation Scheme Operation and MaintenanceNiong DavidPas encore d'évaluation
- Structures For Water Control and DistributionDocument76 pagesStructures For Water Control and Distributionnour100% (2)
- Manual 1 - Introduction To IrrigationDocument152 pagesManual 1 - Introduction To IrrigationNiong DavidPas encore d'évaluation
- Manual 1 - Introduction To IrrigationDocument152 pagesManual 1 - Introduction To IrrigationNiong DavidPas encore d'évaluation
- 43 00 00 - LPG InstallationDocument13 pages43 00 00 - LPG InstallationNiong David100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Community Health Nursing ExamDocument24 pagesCommunity Health Nursing ExamClarisse SampangPas encore d'évaluation
- Inpatient Handbook 2008-2009 UCLADocument275 pagesInpatient Handbook 2008-2009 UCLAartig44Pas encore d'évaluation
- Analisis Sistem Penyelenggaraan Rekam Medis Di Unit Rekam Medis Puskesmas Kota Wilayah Utara Kota KediriDocument7 pagesAnalisis Sistem Penyelenggaraan Rekam Medis Di Unit Rekam Medis Puskesmas Kota Wilayah Utara Kota Kedirikiki naniPas encore d'évaluation
- Study On Functional Outcome of Bimalleolar Ankle FDocument8 pagesStudy On Functional Outcome of Bimalleolar Ankle Fbhushan adhariPas encore d'évaluation
- Koch 2016Document7 pagesKoch 2016Derri PraPas encore d'évaluation
- ADHD Symptomatology Is Best Conceptualized As A Spectrum: A Dimensional Versus Unitary Approach To DiagnosisDocument82 pagesADHD Symptomatology Is Best Conceptualized As A Spectrum: A Dimensional Versus Unitary Approach To DiagnosisPSIQUIATRÍA HUFAPas encore d'évaluation
- Curriculum Vitae: Career ObjectiveDocument2 pagesCurriculum Vitae: Career ObjectiveRajesh Kumar NayakPas encore d'évaluation
- 2020 Case Report Internasional Short Bowel Sindrom Dan BblserDocument6 pages2020 Case Report Internasional Short Bowel Sindrom Dan Bblserdayu mankPas encore d'évaluation
- UNICEF Sri Lanka Humanitarian Situation Report No. 3 (Economic Crisis 2022), 31 December 2022Document11 pagesUNICEF Sri Lanka Humanitarian Situation Report No. 3 (Economic Crisis 2022), 31 December 2022Ada DeranaPas encore d'évaluation
- NURS FPX 6210 Assessment 2 Strategic PlanningDocument6 pagesNURS FPX 6210 Assessment 2 Strategic Planningjoohnsmith070Pas encore d'évaluation
- Updated Unang Yakap Checklist 1Document3 pagesUpdated Unang Yakap Checklist 1Myrel Cedron TucioPas encore d'évaluation
- Hospiatl Malnut PadangDocument36 pagesHospiatl Malnut PadangElvia DesiPas encore d'évaluation
- HA LEC Notes Jan 16 29Document4 pagesHA LEC Notes Jan 16 29Basty BautistaPas encore d'évaluation
- Fullerton Health Sustainability Report FY2022Document76 pagesFullerton Health Sustainability Report FY2022Michael YiinPas encore d'évaluation
- Occupational Health & Safety ReportDocument18 pagesOccupational Health & Safety Reportargya nareswaraPas encore d'évaluation
- Ellen Lent-Wunderlich RN, MS, CPHQ: HighlightsDocument5 pagesEllen Lent-Wunderlich RN, MS, CPHQ: Highlightsapi-2349150Pas encore d'évaluation
- Contract and Agency LawDocument9 pagesContract and Agency Lawdavid omondiPas encore d'évaluation
- A Review On The Oral Health of Pregnant Women Provided With Basic Oral Health Care (BOHC) in The Province of Davao Oriental: A Local PerspectiveDocument17 pagesA Review On The Oral Health of Pregnant Women Provided With Basic Oral Health Care (BOHC) in The Province of Davao Oriental: A Local PerspectiveAudrey Kristina MaypaPas encore d'évaluation
- Quick Guide To Prescribing, Medicine Supplies and Support From Your PharmacyDocument11 pagesQuick Guide To Prescribing, Medicine Supplies and Support From Your Pharmacyminhmap90_635122804Pas encore d'évaluation
- Management of Hepatitis B in Pregnant Women and Infants: A Multicentre Audit From Four London HospitalsDocument8 pagesManagement of Hepatitis B in Pregnant Women and Infants: A Multicentre Audit From Four London HospitalsXenia Marie Razalo LawanPas encore d'évaluation
- MCN - The Childbearing and Childbearing Family in The CommunityDocument91 pagesMCN - The Childbearing and Childbearing Family in The CommunityAndrea Marie SevillaPas encore d'évaluation
- TDM Exam Study Resources PDFDocument5 pagesTDM Exam Study Resources PDFDrosler MedqsPas encore d'évaluation
- EthicsDocument24 pagesEthicsAME DENTAL COLLEGE RAICHUR, KARNATAKAPas encore d'évaluation
- Guide To Clinical AuditDocument54 pagesGuide To Clinical Auditzenti78100% (1)
- Influence of Psychological Stress On Non-Surgical Periodontal Treatment Outcomes in Patients With Severe Chronic PeriodontitisDocument10 pagesInfluence of Psychological Stress On Non-Surgical Periodontal Treatment Outcomes in Patients With Severe Chronic PeriodontitisAndra AgheorghieseiPas encore d'évaluation
- Nbde Study ResourcesDocument3 pagesNbde Study ResourcesMichael GarciaPas encore d'évaluation
- Chen Et Al (2001)Document7 pagesChen Et Al (2001)ayu pathyaPas encore d'évaluation
- Bio Medical WasteDocument6 pagesBio Medical WastePriscilla SolomonPas encore d'évaluation
- Rubric For Drug StudyDocument2 pagesRubric For Drug StudyMart Juaresa Yambao100% (2)
- Essiac A Native Herbal Cancer Remedy Olsen, Cynthia 9781890941000 Books - Amazon - CaDocument1 pageEssiac A Native Herbal Cancer Remedy Olsen, Cynthia 9781890941000 Books - Amazon - CahkvpchdbtpPas encore d'évaluation