Vous aimerez peut-être aussi
- Examination of Body Fluids (Urinalysis)Document109 pagesExamination of Body Fluids (Urinalysis)kiedd_04100% (9)
- Clinical ChemistryDocument26 pagesClinical Chemistryazoooz502Pas encore d'évaluation
- Intro To Medtech Clinical Chemistry ReviewerDocument11 pagesIntro To Medtech Clinical Chemistry Reviewerjesanndei100% (1)
- 13 Biochemical Tests For Gram Negative Bacilli PDFDocument51 pages13 Biochemical Tests For Gram Negative Bacilli PDFSHUPATUSSAIPas encore d'évaluation
- Clinical Bacteriology ReviewerDocument17 pagesClinical Bacteriology Reviewer99noname100% (1)
- Antibody IdentificationDocument74 pagesAntibody IdentificationNilver Zenteno100% (3)
- Group 4 - General Pathology, Logic and Cytologic TechniquesDocument11 pagesGroup 4 - General Pathology, Logic and Cytologic Techniquesjulo_05Pas encore d'évaluation
- ML7111 MCQs Answers April 2020Document16 pagesML7111 MCQs Answers April 2020Cleo SalvadorPas encore d'évaluation
- Urine Screening of Metabolic DisordersDocument24 pagesUrine Screening of Metabolic DisordersMark Arlo Hernandez SegundoPas encore d'évaluation
- Microscopic Examination of UrineDocument4 pagesMicroscopic Examination of UrineGlaiza Erika Baes GudaPas encore d'évaluation
- Plasma Hemoglobin and Urine Hemoglobin EstimationDocument12 pagesPlasma Hemoglobin and Urine Hemoglobin EstimationAvi VermaPas encore d'évaluation
- Blood Banking Course BookDocument2 pagesBlood Banking Course BookShukr Wesman BlbasPas encore d'évaluation
- Group 8 - Microbiology 1 - BacteriologyDocument14 pagesGroup 8 - Microbiology 1 - Bacteriologyjulo_05Pas encore d'évaluation
- Analysis of Urine and Other Body FluidsDocument52 pagesAnalysis of Urine and Other Body FluidsJoseph VillamorPas encore d'évaluation
- Urinalysis and Body Fluids2020Document47 pagesUrinalysis and Body Fluids2020MONFOLA100% (1)
- AUBF Analysis of Urine and Body FluidsDocument581 pagesAUBF Analysis of Urine and Body FluidsQuetzaL coatL100% (1)
- SerologyDocument84 pagesSerologyngsusannasuisum100% (2)
- Anticoagulants and Other PreservativesDocument26 pagesAnticoagulants and Other Preservativessdas317Pas encore d'évaluation
- Stool AnalysisDocument8 pagesStool AnalysisLuciaGomez100% (1)
- Blood Bank ProceduresDocument33 pagesBlood Bank Proceduresninadroy2844100% (20)
- Transfusion Medicine QuestionsDocument31 pagesTransfusion Medicine QuestionsJhoanie Sanggoy Tauli100% (1)
- Clinical Chemistry Review NotesDocument54 pagesClinical Chemistry Review NotesALEONA AMON ARANTEPas encore d'évaluation
- Hema I Chapter 7 - HemocytometryDocument83 pagesHema I Chapter 7 - HemocytometryderibewPas encore d'évaluation
- Biochemical Test of BacteriaDocument33 pagesBiochemical Test of Bacteriaaziskf100% (2)
- Group 1 - Analysis of Urine and Other Body FluidsDocument11 pagesGroup 1 - Analysis of Urine and Other Body Fluidsjulo_05100% (3)
- Hematology Ii Lectures Introduction To HemostasisDocument28 pagesHematology Ii Lectures Introduction To HemostasisJoshua Trinidad100% (1)
- Clinical Chemistry: ToxicologyDocument9 pagesClinical Chemistry: ToxicologyChristine BadilloPas encore d'évaluation
- AUB - Urine Screening For Metabolic DisordersDocument3 pagesAUB - Urine Screening For Metabolic DisordersJeanne Rodiño100% (1)
- Lab ValuesDocument5 pagesLab Valuespragya_devkotaPas encore d'évaluation
- LN Hematology MLT FinalDocument549 pagesLN Hematology MLT FinalMahfuzur Rahman100% (3)
- Diagnostic Bacteriology-Lab ReviewDocument45 pagesDiagnostic Bacteriology-Lab ReviewAtiya HajjajPas encore d'évaluation
- Forward and ReverseDocument11 pagesForward and ReversecyrhenmiePas encore d'évaluation
- Clinical Laboratory Science Review by Theriot - JarreauDocument12 pagesClinical Laboratory Science Review by Theriot - JarreauJuneya Koo100% (1)
- Urinalysis and Body Fluids Q & ADocument79 pagesUrinalysis and Body Fluids Q & ADarla YsavelPas encore d'évaluation
- Practice Questions 1Document12 pagesPractice Questions 1Cha100% (1)
- Enterobacter QuizDocument8 pagesEnterobacter QuizDan Paolo Sanchez100% (2)
- Biochemical TestDocument13 pagesBiochemical TestSusi100% (1)
- Blood Grouping TecheniquesDocument19 pagesBlood Grouping TecheniquesLIBIN PALLUPPETTAYIL JOSE93% (15)
- (Microbio) Staphyloccocus and Streptococcus-Dr. Salandanan (BHND)Document16 pages(Microbio) Staphyloccocus and Streptococcus-Dr. Salandanan (BHND)Lee Delos Santos100% (1)
- Laboratory Dha Praparation MCQ 1-2700Document263 pagesLaboratory Dha Praparation MCQ 1-2700Laal Shirt100% (1)
- Donor Screening and Component PreparationDocument91 pagesDonor Screening and Component PreparationDominic BernardoPas encore d'évaluation
- 8.nature of Clinical Laboratory - EditedDocument56 pages8.nature of Clinical Laboratory - EditedJr BalagtasPas encore d'évaluation
- Micro Lab Prac - PDCR PDFDocument10 pagesMicro Lab Prac - PDCR PDFPatti Danielle Referente50% (2)
- Clinical Chemistry Notes With BlanksDocument34 pagesClinical Chemistry Notes With Blanksepson printerPas encore d'évaluation
- Review in Clinical MicrosDocument103 pagesReview in Clinical MicrosSyvelmarie Tinte100% (1)
- Medical Laboratory Science Post Basic CurriculumDocument187 pagesMedical Laboratory Science Post Basic CurriculumNigusse Obse100% (4)
- Analysis of UrineDocument5 pagesAnalysis of UrineHaridha ChandranPas encore d'évaluation
- Histopathology Chapter 2Document141 pagesHistopathology Chapter 2Zelalem Dejazmach100% (2)
- Must To Know MTLDocument15 pagesMust To Know MTLMae MacalandaPas encore d'évaluation
- Hematology Special StainDocument28 pagesHematology Special Stainandreea0dey100% (1)
- CH 1 2 3 4-5-Professional EthicsDocument81 pagesCH 1 2 3 4-5-Professional EthicsAhmadin Bamud100% (1)
- C1 IH Lab L3 ABO Forward Reverse Typing Manual and Gel MethodDocument8 pagesC1 IH Lab L3 ABO Forward Reverse Typing Manual and Gel MethodDIVINA KYLE YGOPas encore d'évaluation
- Clinical Microscopy ExamDocument3 pagesClinical Microscopy ExamKarla GiorlaPas encore d'évaluation
- Clinical Microscopy: Definition and Volume Disease and Cause PolyuriaDocument5 pagesClinical Microscopy: Definition and Volume Disease and Cause PolyuriaJovanni andesPas encore d'évaluation
- By: Dr. Yoavita Moderator: Dr. Anik Widijanti, SP - PK (K)Document61 pagesBy: Dr. Yoavita Moderator: Dr. Anik Widijanti, SP - PK (K)Gilang KusdinarPas encore d'évaluation
- Urine ComponentsDocument31 pagesUrine ComponentsLarry MagwegwePas encore d'évaluation
- Urine-Analysis 140420Document74 pagesUrine-Analysis 140420sabao kizuitePas encore d'évaluation
- Unit 6 UrineDocument131 pagesUnit 6 UrineAsjad HassanPas encore d'évaluation
- URINALYSISDocument80 pagesURINALYSISredr7131Pas encore d'évaluation
- From The Bodies of Bees Classical and Christian Echoes in Surah Al-NahlDocument25 pagesFrom The Bodies of Bees Classical and Christian Echoes in Surah Al-Nahlkiedd_04Pas encore d'évaluation
- SYNAPSEDocument35 pagesSYNAPSEkiedd_04100% (3)
- "Traditional" Exegeses of Q 4:34Document15 pages"Traditional" Exegeses of Q 4:34kiedd_04Pas encore d'évaluation
- Iklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012Document2 pagesIklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012kiedd_04Pas encore d'évaluation
- The Place For Others in IslamDocument27 pagesThe Place For Others in Islamkiedd_04Pas encore d'évaluation
- Odors of Santity Distinctions of The Holy in Early Christianity and IslamDocument13 pagesOdors of Santity Distinctions of The Holy in Early Christianity and Islamkiedd_04100% (1)
- Refleks ArcsDocument34 pagesRefleks Arcskiedd_04100% (1)
- Fadhilat Surah at TakwirDocument1 pageFadhilat Surah at Takwirkiedd_04Pas encore d'évaluation
- Cell PhysiologyDocument61 pagesCell Physiologykiedd_04100% (4)
- Microbiology Colour Plate No.8Document1 pageMicrobiology Colour Plate No.8kiedd_04Pas encore d'évaluation
- Microbiology Colour Plate No.6Document1 pageMicrobiology Colour Plate No.6kiedd_04Pas encore d'évaluation
- API® CoryneDocument4 pagesAPI® Corynekiedd_04Pas encore d'évaluation
- Microbiology Colour Plate No.7Document1 pageMicrobiology Colour Plate No.7kiedd_04Pas encore d'évaluation
- Microbiology Colour Plate No.4Document1 pageMicrobiology Colour Plate No.4kiedd_04Pas encore d'évaluation
- Microbiology Colour Plate No.3Document1 pageMicrobiology Colour Plate No.3kiedd_04Pas encore d'évaluation
- Microbiology Colour Plate No.9Document1 pageMicrobiology Colour Plate No.9kiedd_04Pas encore d'évaluation
- Microbiology Colour Plate No.5Document1 pageMicrobiology Colour Plate No.5kiedd_04Pas encore d'évaluation
- Microbiology Colour Plate No.1Document1 pageMicrobiology Colour Plate No.1kiedd_04Pas encore d'évaluation
- Microbiology Colour Plate No.2Document1 pageMicrobiology Colour Plate No.2kiedd_04Pas encore d'évaluation
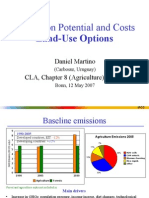
- Mitigation Potential and Costs Land-Use OptionsDocument9 pagesMitigation Potential and Costs Land-Use Optionskiedd_04Pas encore d'évaluation
- Mitigation of Climate ChangeDocument41 pagesMitigation of Climate Changekiedd_04Pas encore d'évaluation
- Philosophical Consolation in Christianity and Islam Boethious and Al-KindiDocument10 pagesPhilosophical Consolation in Christianity and Islam Boethious and Al-Kindikiedd_04Pas encore d'évaluation
- Carnitine DeficiencyDocument21 pagesCarnitine Deficiencykiedd_04100% (1)
- Mitigation of Climate ChangeDocument25 pagesMitigation of Climate Changekiedd_04Pas encore d'évaluation
- Advance Diagnostic Medical Laboratory: The AP 20E® For Identification of BacteriaDocument1 pageAdvance Diagnostic Medical Laboratory: The AP 20E® For Identification of Bacteriakiedd_04100% (1)
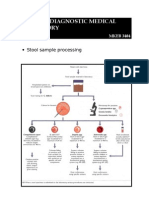
- Stool Sample ProcessingDocument1 pageStool Sample Processingkiedd_04Pas encore d'évaluation
- Oxidase TestDocument1 pageOxidase Testkiedd_04100% (1)
- Diagram of Classification of EnterobacteriaDocument1 pageDiagram of Classification of Enterobacteriakiedd_04100% (1)
- The Differential Cell CountDocument12 pagesThe Differential Cell Countariel100% (1)
- Journal Homepage: - : IntroductionDocument5 pagesJournal Homepage: - : IntroductionIJAR JOURNALPas encore d'évaluation
- SOP - Handling AsbestosDocument61 pagesSOP - Handling AsbestosAndre MarsPas encore d'évaluation
- Rapport Om Chemical ContaminantsDocument181 pagesRapport Om Chemical Contaminantsacestre10Pas encore d'évaluation
- Surgical Treatment For Colorectal CancerDocument3 pagesSurgical Treatment For Colorectal CancerOwais ArifPas encore d'évaluation
- IsoWhey ArticlesDocument4 pagesIsoWhey ArticlesLynnemax100% (2)
- Introductory Paragraphs-PresentationDocument24 pagesIntroductory Paragraphs-PresentationManal SalamehPas encore d'évaluation
- Embark Results SarahDocument10 pagesEmbark Results Sarahapi-399849391Pas encore d'évaluation
- Rituximab MonographDocument11 pagesRituximab MonographIrma Nurtiana SyafitriPas encore d'évaluation
- Parotid LabDocument11 pagesParotid Labapi-268707929Pas encore d'évaluation
- Detecting and Recognising Lung Cancer: Using Convolutional Neural NetworksDocument25 pagesDetecting and Recognising Lung Cancer: Using Convolutional Neural NetworksRAJU MAURYAPas encore d'évaluation
- Asymptomatic Hyperuricemia: To Treat or Not To Treat: ReviewDocument8 pagesAsymptomatic Hyperuricemia: To Treat or Not To Treat: ReviewkkichaPas encore d'évaluation
- Cancer Statistics, 2011: The Impact of Eliminating Socioeconomic and Racial Disparities On Premature Cancer DeathsDocument25 pagesCancer Statistics, 2011: The Impact of Eliminating Socioeconomic and Racial Disparities On Premature Cancer DeathshamzaloPas encore d'évaluation
- Malignancy Yield of Testis PathologyDocument7 pagesMalignancy Yield of Testis PathologyadolfoPas encore d'évaluation
- PSAvs PsadDocument6 pagesPSAvs PsadRaga ManduaruPas encore d'évaluation
- Smoothelin (R4A) - CM - MAN - EN - IVD - 1.0 PDFDocument5 pagesSmoothelin (R4A) - CM - MAN - EN - IVD - 1.0 PDFOlteanu Gheorghe-EmilianPas encore d'évaluation
- Abstrak Medika Mentosa PDFDocument3 pagesAbstrak Medika Mentosa PDFpawiroPas encore d'évaluation
- Destructive OperationDocument8 pagesDestructive OperationNishaThakuri100% (4)
- Once Again A Vegan Centenarian Is The Nation's Oldest Man! - 112 Year Old Pandit Sudhakar Chaturvedi - Not Paleo, Low Carb, Wheat Belly, Atkins, But VegetarianDocument3 pagesOnce Again A Vegan Centenarian Is The Nation's Oldest Man! - 112 Year Old Pandit Sudhakar Chaturvedi - Not Paleo, Low Carb, Wheat Belly, Atkins, But VegetarianPaleoCentenarianDiet33% (3)
- Clinical Surgery in General RCS Course ManualDocument2 pagesClinical Surgery in General RCS Course ManualsafiPas encore d'évaluation
- Goljan Errata SheetDocument11 pagesGoljan Errata SheetVishala MishraPas encore d'évaluation
- Different Kinds of PhobiasDocument3 pagesDifferent Kinds of PhobiasLajila100% (1)
- Garcinia Kola ThesisDocument36 pagesGarcinia Kola ThesisDdn RmaPas encore d'évaluation
- Managemant Copd CPG MsiaDocument67 pagesManagemant Copd CPG MsiaNur Anis ZarimePas encore d'évaluation
- Steroid Tapering and Supportive Treatment Guidance V1.0 PDFDocument1 pageSteroid Tapering and Supportive Treatment Guidance V1.0 PDFNthutagaol TrusPas encore d'évaluation
- Genetic DisordersDocument2 pagesGenetic DisordersEzekiel Arteta100% (2)
- EAT-Lancet Is A FraudDocument4 pagesEAT-Lancet Is A FraudAnonymous BWVVQpxPas encore d'évaluation
- Case Study (Nasopharyngeal Cancer)Document31 pagesCase Study (Nasopharyngeal Cancer)aj christian93% (15)
- Skin Nail HairDocument48 pagesSkin Nail HairkitsilcPas encore d'évaluation
- VertigoDocument3 pagesVertigoAacg MeryendPas encore d'évaluation