Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Accounting Information System - Chapter 1Document41 pagesAccounting Information System - Chapter 1Lizette OlivaPas encore d'évaluation
- ThreatDocument1 pageThreatjunejune1793Pas encore d'évaluation
- AIS01Document49 pagesAIS01Fitriyah Az-zahraaPas encore d'évaluation
- 2012 AICPA Financial QuestionsDocument60 pages2012 AICPA Financial Questionsjunejune1793Pas encore d'évaluation
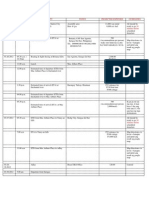
- Date Time Activity Venue Projected Expenses GuidelinesDocument1 pageDate Time Activity Venue Projected Expenses Guidelinesjunejune1793Pas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Dvanced Cardiac Life SupportDocument72 pagesDvanced Cardiac Life Supportolivia100% (1)
- EpinephrineDocument4 pagesEpinephrinegovind_soni_15Pas encore d'évaluation
- Pha-Bls 2H2019Document3 pagesPha-Bls 2H2019Abram BunoanPas encore d'évaluation
- Acls FixDocument20 pagesAcls Fixluthfi adityaPas encore d'évaluation
- BLS For TeacherrDocument166 pagesBLS For TeacherrGavinKarl Mianabanatao100% (1)
- MylatestSOS BLS ACLS LectureDocument87 pagesMylatestSOS BLS ACLS LectureArmin MercadoPas encore d'évaluation
- CPR MCQ 03Document21 pagesCPR MCQ 03Ryam Taif100% (1)
- 2013 Eman Ramadan Abdel Moniem AliDocument5 pages2013 Eman Ramadan Abdel Moniem AliEug UlepPas encore d'évaluation
- Philippine Heart AssociationDocument2 pagesPhilippine Heart AssociationNURSES' PADPas encore d'évaluation
- Rahal ResumeDocument2 pagesRahal Resumeapi-503911568Pas encore d'évaluation
- Approved Abbreviations: Administrative 1.0Document12 pagesApproved Abbreviations: Administrative 1.0jhoniPas encore d'évaluation
- User Manual CardiostartDocument113 pagesUser Manual CardiostartLouie Jay AmantePas encore d'évaluation
- Professional Development Plan: By: Isabella RahalDocument10 pagesProfessional Development Plan: By: Isabella Rahalapi-503911568Pas encore d'évaluation
- Basic Life Support (BLS) in AdultsDocument13 pagesBasic Life Support (BLS) in AdultsElena ChitoiuPas encore d'évaluation
- ACLS SubhankarDocument87 pagesACLS SubhankarMarc Andreo MalalaPas encore d'évaluation
- Basic Life Support Written ReportDocument8 pagesBasic Life Support Written ReportLovely Ann AviadoPas encore d'évaluation
- ACLS Precourse Self-AssessmentDocument3 pagesACLS Precourse Self-AssessmentHollan GaliciaPas encore d'évaluation
- Managemen Disritmia: Dr. Rofika Hanifa, SPPDDocument20 pagesManagemen Disritmia: Dr. Rofika Hanifa, SPPDavivlabirdPas encore d'évaluation
- Emergency and Disaster Nursing 2012Document218 pagesEmergency and Disaster Nursing 2012Darran Earl Gowing100% (2)
- ACLS Online Training Material: Unit One: General ConceptsDocument34 pagesACLS Online Training Material: Unit One: General ConceptsJohn JenjinsPas encore d'évaluation
- ACLS Secondary Survey For A Patient in Respiratory ArrestDocument2 pagesACLS Secondary Survey For A Patient in Respiratory ArrestLady MuffinsPas encore d'évaluation
- Emergency Cart ProcedureDocument20 pagesEmergency Cart ProcedureAyiessa_AJPas encore d'évaluation
- American Heart Association Acls Post Test AnswersDocument4 pagesAmerican Heart Association Acls Post Test AnswersArun Jude Alphonse0% (9)
- Cardiology USMLE 2CK (Cardio Clinical Care) Flashcards - MemorangDocument4 pagesCardiology USMLE 2CK (Cardio Clinical Care) Flashcards - MemorangMohamed Abbas0% (2)
- AHA Program Administration ManualDocument69 pagesAHA Program Administration ManualMohammad AbdUllah TahirPas encore d'évaluation
- AclsDocument13 pagesAclsAllah YarPas encore d'évaluation
- 12 - Chapter 2Document39 pages12 - Chapter 2Add KPas encore d'évaluation
- Pals Pediatric BradycardiaDocument1 pagePals Pediatric BradycardiadarlingcarvajalduquePas encore d'évaluation
- Management of Cardiac ArrestDocument10 pagesManagement of Cardiac ArrestAhmed VelićPas encore d'évaluation
- Updatesincardiacarrest Resuscitation: Vivian Lam,, Cindy H. HsuDocument15 pagesUpdatesincardiacarrest Resuscitation: Vivian Lam,, Cindy H. HsuFia Bella KusumaPas encore d'évaluation