Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Journey To A DiagnosisDocument4 pagesJourney To A DiagnosisMark HayesPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- CertificateDocument1 pageCertificateDrazarPas encore d'évaluation
- JOURNALDocument3 pagesJOURNALAngela NeriPas encore d'évaluation
- Khat Factsheet - 020914 PDFDocument2 pagesKhat Factsheet - 020914 PDFMohammedOumerPas encore d'évaluation
- RO-INMED 2016 ProgramDocument18 pagesRO-INMED 2016 Programmamulasioan9675Pas encore d'évaluation
- Airway Management - CHFDocument2 pagesAirway Management - CHFRindang_Citraw_1819Pas encore d'évaluation
- Medigroup Proposal For ICU BedsDocument13 pagesMedigroup Proposal For ICU Bedsmohyeb padamshiPas encore d'évaluation
- About Tattoos What Is A Tattoo?Document2 pagesAbout Tattoos What Is A Tattoo?Çağatay SarıkayaPas encore d'évaluation
- Consent FormsDocument2 pagesConsent FormsKristeline MedelPas encore d'évaluation
- Unit 55Document7 pagesUnit 55Antara BiswasPas encore d'évaluation
- Pengaruh Deep Breathing Terhadap Kecemasan Pra OperasiDocument14 pagesPengaruh Deep Breathing Terhadap Kecemasan Pra OperasiAch ThungPas encore d'évaluation
- Eurohealth 28 1 2022 EngDocument64 pagesEurohealth 28 1 2022 EngFitriPas encore d'évaluation
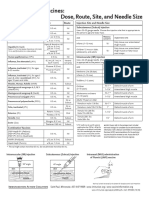
- Injection Site and Needle Size Vaccine Dose RouteDocument1 pageInjection Site and Needle Size Vaccine Dose RouteDr Ambana GowdaPas encore d'évaluation
- Pre-op Evaluation SummaryDocument1 pagePre-op Evaluation Summarysabbo morsPas encore d'évaluation
- Measuring Disease Occurrence and Causal EffectsDocument4 pagesMeasuring Disease Occurrence and Causal EffectsTrần Khải VănPas encore d'évaluation
- HEALTHCARE Prelims TOPIC 3.1-4 Lecture NotesDocument4 pagesHEALTHCARE Prelims TOPIC 3.1-4 Lecture NotesMa. Loucel RodriguezPas encore d'évaluation
- Fever and RashDocument14 pagesFever and RashwirdahajaPas encore d'évaluation
- COVIDDocument13 pagesCOVIDStephen RomeroPas encore d'évaluation
- Reflective Journal 1Document4 pagesReflective Journal 1api-365605511Pas encore d'évaluation
- The National AIDS Council in Collaboration With The Ministry of Primary and Secondary 2018 QuizDocument7 pagesThe National AIDS Council in Collaboration With The Ministry of Primary and Secondary 2018 QuizFelistus TemboPas encore d'évaluation
- Euthanasia and Assisted SuicideDocument14 pagesEuthanasia and Assisted Suicideapi-314071146Pas encore d'évaluation
- HPV: Infection, Prevention and Vaccination in India: Ritesh KumarDocument6 pagesHPV: Infection, Prevention and Vaccination in India: Ritesh Kumarsandeep raiPas encore d'évaluation
- Sanford Chris CVDocument9 pagesSanford Chris CVChris SanfordPas encore d'évaluation
- Luis Andres Arcos Montoya 2014Document11 pagesLuis Andres Arcos Montoya 2014luisandresarcosPas encore d'évaluation
- Allen - Chap - 1 - Art, Science and Technology of Pharmaceutical Compounding, 4eDocument18 pagesAllen - Chap - 1 - Art, Science and Technology of Pharmaceutical Compounding, 4enephylymPas encore d'évaluation
- Ujian Patol B 21/10/2022: A. 2500 ML B. 3200 ML C. 4500 ML D. 5000 MLDocument4 pagesUjian Patol B 21/10/2022: A. 2500 ML B. 3200 ML C. 4500 ML D. 5000 MLBernas Arion NapitupuluPas encore d'évaluation
- Data Master DiagnosaDocument40 pagesData Master Diagnosabagoang puskesmasPas encore d'évaluation
- Dental Caries: Diagnosis and Treatment OptionsDocument53 pagesDental Caries: Diagnosis and Treatment OptionsDaniel WangPas encore d'évaluation
- Assignment On Field Appraisal ReportDocument5 pagesAssignment On Field Appraisal ReportRenita ChrisPas encore d'évaluation
- Thyroid Disorders Part II Hypothyroidism and Thyroiditis LIttle 2006Document6 pagesThyroid Disorders Part II Hypothyroidism and Thyroiditis LIttle 2006Jing XuePas encore d'évaluation