Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Improve posture and movement with the Alexander techniqueDocument7 pagesImprove posture and movement with the Alexander techniquedrdivish100% (4)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Being Single Vs Being MarriedDocument34 pagesBeing Single Vs Being MarriedPeter MissolePas encore d'évaluation
- Abpmr Moc100Document43 pagesAbpmr Moc100Zeeshan Siddiqui100% (4)
- Geriatrics Prescribing GuidelinessDocument27 pagesGeriatrics Prescribing GuidelinessSayli Gore100% (1)
- Lower Gastrointestinal Bleeding: Practice EssentialsDocument28 pagesLower Gastrointestinal Bleeding: Practice EssentialsJohnPaulOliverosPas encore d'évaluation
- 2016 MD Bond-$200k To Damascus HS Boosters For ArtTurfDocument5 pages2016 MD Bond-$200k To Damascus HS Boosters For ArtTurfConcussion_MCPS_MdPas encore d'évaluation
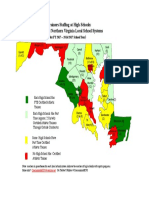
- Projected Athletic Trainer Staffing in FY 2017-Md, NoVA, and DCDocument1 pageProjected Athletic Trainer Staffing in FY 2017-Md, NoVA, and DCConcussion_MCPS_MdPas encore d'évaluation
- LCPS Response To Parents Re Inova-Brain Sentry Research ProposalDocument2 pagesLCPS Response To Parents Re Inova-Brain Sentry Research ProposalConcussion_MCPS_MdPas encore d'évaluation
- MCPS Chart Showing Sports Concussions by Sport and by High School 2013-2014Document1 pageMCPS Chart Showing Sports Concussions by Sport and by High School 2013-2014Concussion_MCPS_MdPas encore d'évaluation
- MCPS Ath Trainer Staffing-FY2016 OpBdgt Summary P 40 of 73Document73 pagesMCPS Ath Trainer Staffing-FY2016 OpBdgt Summary P 40 of 73Concussion_MCPS_MdPas encore d'évaluation
- MCPS Systemwide Safety PRGM - Employee Injury Report 01-16-2014Document9 pagesMCPS Systemwide Safety PRGM - Employee Injury Report 01-16-2014Concussion_MCPS_MdPas encore d'évaluation
- Parent Letter To MCPS Re Student Injury Data - 01-14-2015Document11 pagesParent Letter To MCPS Re Student Injury Data - 01-14-2015Concussion_MCPS_MdPas encore d'évaluation
- MCPS Sports Concussion Data 2014-15Document1 pageMCPS Sports Concussion Data 2014-15Concussion_MCPS_MdPas encore d'évaluation
- MCPS Sports Concussion Data 2013-14Document1 pageMCPS Sports Concussion Data 2013-14Concussion_MCPS_MdPas encore d'évaluation
- NFL 2010 Letter Re Concussion LegDocument2 pagesNFL 2010 Letter Re Concussion LegConcussion_MCPS_MdPas encore d'évaluation
- MCPS Response-Data Re Concussion and Other Injuries in High School Athletics 2013-2014Document2 pagesMCPS Response-Data Re Concussion and Other Injuries in High School Athletics 2013-2014Concussion_MCPS_MdPas encore d'évaluation
- Brain Sentry Inova Football Helmet Sensor Research Study ProposalDocument5 pagesBrain Sentry Inova Football Helmet Sensor Research Study ProposalConcussion_MCPS_MdPas encore d'évaluation
- MCPS (MD) Penalties For Tobacco Use at SchoolDocument2 pagesMCPS (MD) Penalties For Tobacco Use at SchoolConcussion_MCPS_MdPas encore d'évaluation
- MCPS Staff Response To MoCo BOE Durso Q Re Concussion Jan-Feb 2014Document2 pagesMCPS Staff Response To MoCo BOE Durso Q Re Concussion Jan-Feb 2014Concussion_MCPS_MdPas encore d'évaluation
- MCPS (MD) Parent Request For Sports Injuries Data 06-03-2014Document6 pagesMCPS (MD) Parent Request For Sports Injuries Data 06-03-2014Concussion_MCPS_MdPas encore d'évaluation
- Minutes of MD ST BD of Ed Meeting, 4-22-2014Document47 pagesMinutes of MD ST BD of Ed Meeting, 4-22-2014Concussion_MCPS_MdPas encore d'évaluation
- PPE Ath W/ Special Needs-Suppl History FormDocument1 pagePPE Ath W/ Special Needs-Suppl History FormConcussion_MCPS_MdPas encore d'évaluation
- MCPS (MD) Tobacco-Free SCH PolicyDocument2 pagesMCPS (MD) Tobacco-Free SCH PolicyConcussion_MCPS_MdPas encore d'évaluation
- MPSSAA HeadsUp Media Release, 5-5-2014Document1 pageMPSSAA HeadsUp Media Release, 5-5-2014Concussion_MCPS_MdPas encore d'évaluation
- Template 3-B, MCPS Athletics Injury Report-11 High School (From Athletic Trainer Data)Document1 pageTemplate 3-B, MCPS Athletics Injury Report-11 High School (From Athletic Trainer Data)Concussion_MCPS_MdPas encore d'évaluation
- Template 1-C, MCPS 25 High Schools Athletics Injury Report, 2013-2014Document2 pagesTemplate 1-C, MCPS 25 High Schools Athletics Injury Report, 2013-2014Concussion_MCPS_MdPas encore d'évaluation
- Template 3-A, MCPS Athletics Injury Report Each High School (From Athletic Trainer Data)Document1 pageTemplate 3-A, MCPS Athletics Injury Report Each High School (From Athletic Trainer Data)Concussion_MCPS_MdPas encore d'évaluation
- MCPS Systemwide Safety PRGM - Employee Injury Report 01-16-2014Document9 pagesMCPS Systemwide Safety PRGM - Employee Injury Report 01-16-2014Concussion_MCPS_MdPas encore d'évaluation
- Template 2-B, MCPS 25 High Schools Athletics Concussion Database Report, July 2013 - June 2014Document1 pageTemplate 2-B, MCPS 25 High Schools Athletics Concussion Database Report, July 2013 - June 2014Concussion_MCPS_MdPas encore d'évaluation
- Template 1-B, MCPS Athletics Injury Reports 2013-2014Document2 pagesTemplate 1-B, MCPS Athletics Injury Reports 2013-2014Concussion_MCPS_MdPas encore d'évaluation
- HoCo MD BOE Agenda 01-23-14Document2 pagesHoCo MD BOE Agenda 01-23-14Concussion_MCPS_MdPas encore d'évaluation
- Template 2-A, MCPS XXX High School Athletics Concussion Database Report, July 2013 - June 2014Document1 pageTemplate 2-A, MCPS XXX High School Athletics Concussion Database Report, July 2013 - June 2014Concussion_MCPS_MdPas encore d'évaluation
- Template 1-A, MCPS Student Accident Report Injuries 7-1-2013-PresentDocument1 pageTemplate 1-A, MCPS Student Accident Report Injuries 7-1-2013-PresentConcussion_MCPS_MdPas encore d'évaluation
- MCPS Reg For Reporting Student InjuriesDocument2 pagesMCPS Reg For Reporting Student InjuriesConcussion_MCPS_MdPas encore d'évaluation
- MCPS Student Injury Report FormDocument2 pagesMCPS Student Injury Report FormConcussion_MCPS_MdPas encore d'évaluation
- PSW Weclome LetterDocument5 pagesPSW Weclome LetterMallius AllerisPas encore d'évaluation
- Form 1 LHS ML Info1 Monitoring Summary FormDocument3 pagesForm 1 LHS ML Info1 Monitoring Summary FormHarold Paulo MejiaPas encore d'évaluation
- Hydroxychloroquine and Azithromycin As A Treatment of COVID-19Document6 pagesHydroxychloroquine and Azithromycin As A Treatment of COVID-19Larissa ChaveirinhoPas encore d'évaluation
- Successful Strategy To Decrease Indwelling Catheter Utilization Rates inDocument7 pagesSuccessful Strategy To Decrease Indwelling Catheter Utilization Rates inWardah Fauziah El SofwanPas encore d'évaluation
- Longevity Anti-Senescence Therapy Global BCC 2019Document128 pagesLongevity Anti-Senescence Therapy Global BCC 2019Saulius BarauskasPas encore d'évaluation
- Report On Progress of Professional Portfolio - NFDN 1002Document2 pagesReport On Progress of Professional Portfolio - NFDN 1002api-317607382Pas encore d'évaluation
- Laws and policies against cigarette smokingDocument16 pagesLaws and policies against cigarette smokingHarlene Dela Cruz OzarPas encore d'évaluation
- Major Case Presentation On Acute Pulmonary Embolism WithDocument13 pagesMajor Case Presentation On Acute Pulmonary Embolism WithPratibha NatarajPas encore d'évaluation
- Akhil Kumar Ramesh Halpani: Organization Structure Training AT Sukraft Recycling PVT Ltd. (Satari, Goa)Document35 pagesAkhil Kumar Ramesh Halpani: Organization Structure Training AT Sukraft Recycling PVT Ltd. (Satari, Goa)Akhil PatelPas encore d'évaluation
- MortuaryDocument6 pagesMortuaryDr.Rajesh KamathPas encore d'évaluation
- Understanding Literature SynthesisDocument5 pagesUnderstanding Literature SynthesisJimboy MaglonPas encore d'évaluation
- Health & SafetyDocument6 pagesHealth & Safetykamran alamPas encore d'évaluation
- Name: Eric P. Alim Year & Section: CMT-1Document27 pagesName: Eric P. Alim Year & Section: CMT-1Ariel BobisPas encore d'évaluation
- Sample Employee Stress QuestionnaireDocument1 pageSample Employee Stress Questionnairesanthosh222250% (2)
- Principles of Case Planning in Social Work PracticeDocument4 pagesPrinciples of Case Planning in Social Work PracticeJane GilgunPas encore d'évaluation
- Philippines Volume 10 FernDocument2 pagesPhilippines Volume 10 FernJen Aquino ZetaPas encore d'évaluation
- The Many Faces of LeadershipDocument6 pagesThe Many Faces of LeadershipbillpaparounisPas encore d'évaluation
- Medical BacteriologyDocument108 pagesMedical BacteriologyTamarah YassinPas encore d'évaluation
- Bac Level: Beer Is A Beverage FermentedDocument2 pagesBac Level: Beer Is A Beverage FermentedBea ToletePas encore d'évaluation
- Health and SafetyDocument26 pagesHealth and SafetyReza NugrahaPas encore d'évaluation
- TRACTIONDocument3 pagesTRACTIONCatherinePas encore d'évaluation
- Trichiasis: Prepared By:pooja Adhikari Roll No.: 27 SMTCDocument27 pagesTrichiasis: Prepared By:pooja Adhikari Roll No.: 27 SMTCsushma shresthaPas encore d'évaluation
- 2020 What Is Arthritis 15 1Document32 pages2020 What Is Arthritis 15 1Oana BordeianuPas encore d'évaluation
- ACN 3 Knowledge Regarding Water Born Diseases and Its PreventionDocument5 pagesACN 3 Knowledge Regarding Water Born Diseases and Its PreventionFouzia GillPas encore d'évaluation
- MikmikDocument2 pagesMikmikMaria Mikaela PelagioPas encore d'évaluation